Beyond the “Quick Fix”: 7 Radical Shifts to Reclaim Your Metabolic and Mental Sovereignty After 35
Modern life is a biological mismatch, a quiet fracture running through the very soul of our evolutionary design. We exist in a world of ultra-processed chaos, surrounded by industrial “non-foods” engineered with clinical precision to bypass our satiety signals and hijack our dopamine pathways. This is not merely a physiological crisis; it is an emotional drain that robs you of the energy required for your family, your career, and your self-actualisation. You have likely been conditioned to accept a baseline of fatigue, brain fog, and “middle-age spread” as an inevitable part of ageing. It is time to face the truth: these are not signs of getting older; they are correctable symptoms of a broken environment and a hijacked biology.
If you are over 35, you have probably noticed that the margin for error has narrowed. Your body no longer “bounces back” from a weekend of industrial inputs. You feel “stuck”—waking up tired regardless of hours slept, struggling with weight that resists traditional exercise, and lying to yourself so convincingly that you almost believe everything is “fine.” But when the world is quiet at night, the truth claws at your ribs. You look in the mirror and don’t recognise the face staring back. You feel like a hostage to the industrial food complex, trapped in a cycle of inflammation and exhaustion.
This document is your clinical-grade exit strategy. It is the path to Metabolic Sovereignty—the reclamation of your body and mind from industrial and neurological control. We are going to dismantle the “biological mismatch” by marrying the heart-healthy, lipid-rich traditions of the Mediterranean with the rigorous ancestral boundaries of the Paleo framework. This is about more than “losing weight”; it is about rebuilding your energy from the cellular level up and becoming the person you were always meant to become.
——————————————————————————–
1. What is the Insulin Lock? How to Reverse Glucose Dependency After 35
To reclaim your health, you must transition from being “glucose-dependent” to achieving “Metabolic Flexibility.” This is the evolutionary ability to switch seamlessly between burning the energy from your food (glucose) and burning the energy stored in your body fat. Most modern adults have lost this ability due to a phenomenon known as the Insulin Lock.
Insulin is your primary storage hormone. Every time you consume wheat, pasta, refined sugar, or excessive starch, your blood glucose spikes. In response, your pancreas floods the system with insulin to clear the sugar. The problem is that when insulin levels are high, your fat cells are biochemically “locked.” High insulin levels inhibit the enzyme Hormone-Sensitive Lipase (HSL), which is the master switch required to break down body fat for fuel.
“Even if you carry 50,000 calories of energy on your body, your brain thinks you are starving because the fuel is behind a locked door.” — Ian Callaghan.
When you are glucose-dependent, you are essentially a hybrid car that has forgotten how to use its electric battery, constantly stopping for petrol every two hours. Your brain, sensing that it cannot access its fat stores, sends out emergency hunger signals. This is why you feel shaky, irritable, and “hangry” shortly after a high-carb meal. By lowering your baseline insulin, we allow your body to “turn the key” and access its own massive energy stores. As insulin falls, your brain’s sensitivity to Leptin—your master satiety hormone—is restored. You finally feel full, often for the first time in decades, because the “insulin noise” is no longer blocking the signal that you have plenty of fuel.
——————————————————————————–
2. Why Willpower Fails: How to Fix a Slow Metabolism Through Identity
Traditional “dieting” is a temporary state of misery; a period of restriction followed by an inevitable return to “normal.” But for the mature adult, “normal” is exactly what caused the dysfunction. In the pursuit of Metabolic Sovereignty, we do not use the word “diet.” Instead, we establish Standards.
Willpower is an unstable, finite resource. It fluctuates with your sleep quality, your stress levels, and your blood sugar. It is a neurological battery that drains throughout the day, which is why most relapses happen at 8:00 PM on a Tuesday, not 8:00 AM on a Monday. Identity, however, is steady. Your brain always acts according to who it believes you are.
The Standard vs The Diet
The “Diet” Mindset: A temporary fight against your own biology. It relies on forcing a brain that is still running old “drinker” or “sugar-junkie” software. It feels like a daily battle you are destined to lose.
The “Standard” Mindset: A permanent baseline of quality based on self-respect. It recognises that seed oils and refined sugars are not “food” but chemical inputs. You don’t “miss out” on them; you exercise sovereignty over your system.
Your brain follows “neurological tracks”—deep canyons carved into your grey matter by decades of repetition. You didn’t choose your dependency; your brain simply followed the shortcuts you gave it. Rewiring your mind requires you to stop “trying” to change and start “being” the person who doesn’t consume industrial non-foods. When you align your identity with your actions, the friction disappears. You are no longer “trying to be healthy”; you are simply a person who holds high standards for what enters their temple.
——————————————————————————–
3. What are the Dangers of Seed Oils? Reclaiming the Ancestral Gold Standard
Perhaps the most damaging substance in the modern industrial diet is one frequently marketed as “heart-healthy”: industrial seed oils (rapeseed/canola, sunflower, corn, and soybean oil). These are modern inventions, birthed through high-heat processing, chemical solvents, and industrial deodorisation.
These oils are extremely high in linoleic acid, an omega-6 fatty acid that is fundamentally unstable. When you consume these oils, they don’t just “burn off.” They are incorporated into your cell membranes and stored in your adipose tissue for years.
“Think of these unstable fats like rusted, sparking wiring in a high-voltage system. They don’t just sit there; they can contribute to oxidative ‘sparks’ that damage neighbouring cells and inflame the lining of your arteries.” — Ian Callaghan.
Because they are prone to oxidation, seed oils induce chronic oxidative stress and “oxidative debt.” They interfere with mitochondrial function, making metabolic flexibility nearly impossible. In this framework, we return to the ancestral gold standard: Extra Virgin Olive Oil (EVOO). Rich in polyphenols and stable monounsaturated fats, EVOO supports cardiovascular health and provides the proper signals to your metabolism. It is the literal lubricant for a well-functioning biological machine.
——————————————————————————–
4. How to Silence the “Sugar Dragon” Using the Satiety Triad
To end the cycle of constant grazing and “food noise,” every meal must satisfy the Satiety Triad: Protein, Healthy Fat, and Fibre. If you find yourself hunting for a snack two hours after eating, you have failed to hit the necessary biological thresholds.
The most critical component is the Protein Leverage Effect. Evolutionary biology suggests that the human brain will maintain hunger signals—the “Sugar Dragon”—until a specific threshold of amino acids is met. If you eat low-protein, processed foods, your brain will keep you hungry in a desperate attempt to find the nitrogen and amino acids it needs for repair. By prioritising high-quality proteins like seafood, eggs, and grass-fed meats, you shut down the hunger signal at its source.
The Satiety Triad: Biological Signalling Mechanisms
Component
Biological Signal
Purpose
Protein
Amino Acid Threshold
Triggers the “Protein Leverage Effect” to shut down the hypothalamus’s hunger drive.
Healthy Fat
CCK (Cholecystokinin)
Signals the gallbladder to release bile and tells the brain to relax into a “fed” state.
Fibre
Gastric Distension
Provides physical bulk and feeds gut bacteria (like Akkermansia) to produce short-chain fatty acids.
By focusing on nutrient-dense proteins—specifically sardines, mackerel, and grass-fed beef—you provide your body with the iodine, selenium, and B-vitamins required to keep your “biological furnace” (the thyroid) burning at its peak capacity.
——————————————————————————–
5. Nervous System Regulation: Why “Light and Salt” are Metabolic Signals
Metabolism is not a simple game of calories; it is a downstream result of the state of your nervous system. If your biology believes you are under threat—stuck in a perpetual “fight or flight” loop—it will prioritise glucose storage and systemic inflammation over fat-burning. We must use physical anchors to signal safety to the brain.
The Four Anchors of Sovereignty
Morning Light: Within 30 minutes of waking, get 10 minutes of direct outdoor sunlight. This sets your circadian rhythm, regulating cortisol and ensuring that melatonin is produced at the correct time 16 hours later.
The Mineral Baseline: Drink 500ml of room-temperature water with 1/2 tsp of high-quality sea salt every morning. As insulin drops, your kidneys begin to dump excess water and sodium (often called the “Keto Flu”). This saltwater anchor prevents headaches and fatigue, managing the mineral shift as you transition to a Paleo framework.
Cold Water Resets: A 30-second cold rinse at the end of your shower. This “hormetic stress” stimulates Brown Adipose Tissue (BAT)—the “fat-burning fat” that generates heat and resets the nervous system instantly.
Box Breathing: Use a cycle of 4s in, 4s hold, 4s out, 4s hold. This activates the parasympathetic nervous system—your body’s natural brake pedal—telling your biology that you are safe and can move into “rest and digest” mode.
——————————————————————————–
6. Dismantling the “Triggers”: The 10-Second Rule for Breaking Cravings
You do not “fail” because you are weak; you get ambushed by your own nervous system. Triggers are not logical thoughts; they are lightning-fast neurological reactions buried in your “lizard brain.” They fire before your conscious mind even has a chance to intervene.
To dismantle these landmines, you must understand the timeline of an urge. Neurobiology shows that a craving “spike” generally lasts for approximately 90 seconds. If you can interrupt the neurological loop for just ten seconds, you stop the dopamine-driven “autopilot” from taking the wheel.
The “10-Second Interruption” Protocol
When a trigger hits—be it stress, a certain time of day, or an emotional flash—immediately apply the 4 Questions That Kill Cravings:
What am I actually feeling? (Is this hunger, or is it loneliness, stress, or boredom? Naming the emotion moves the activity from the impulsive amygdala to the rational prefrontal cortex.)
What do I actually need? (Do I need a “non-food” input, or do I need rest, connection, or a mineral reset?)
Will this fix the problem? (The answer is always no; it will only add the weight of shame to the original feeling.)
How will I feel tomorrow? (Will I feel clear-headed and sovereign, or will I be crawling through the fog of a relapse?)
By naming the trigger, you move from “drowning” in the feeling to “observing” it. Observation is the ultimate sovereignty hack.
——————————————————————————–
7. Building the “Legacy Identity”: Self-Creation After 35
After the age of 35, you are no longer just surviving; you are self-creating. You have reached a stage where your physical health is the foundation for your emotional stability and the legacy you leave for your children. This is the Embodiment stage.
“You are not a problem that needs fixing. You are someone who finally reached the point where running hurt more than facing the truth.” — Ian Callaghan.
Building a Legacy Identity means setting standards that your family can follow. It is the recognition that you are the architect of your future. When your identity is “locked in,” you don’t “hope” to stay on track—you simply live as the person who is sober from industrial interference. You are no longer a customer for the pharmaceutical consequences of a broken food system. You have outgrown your old life.
——————————————————————————–
The 28-Day Blueprint: Your Biological Renovation
This reset is structured as a 28-day systematic renovation of your internal factory settings. It is not a buffet; it is a progression.
The 28-Day Structural Progression
Phase
Biological Focus
Primary “Job”
Week 1
Withdrawal & Stabilisation
Breaking the “Sugar Dragon.” Establishing the mineral baseline (Salt/Water) to manage electrolyte shifts.
Week 2
Gut & Inflammation
Healing the gut-mucosal barrier with collagen and re-seeding the microbiome with fermented foods like sauerkraut.
Week 3
Metabolic Flexibility
Mastering meal timing and the “Protein Leverage Effect.” Signalling the body to switch to fat-burning.
Week 4
Consolidation & Sovereignty
Establishing permanent standards and building “social resilience” (learning to say “No” to seed oils).
To hit the word count and provide clinical value, we must look at the specific “Metabolic Sovereignty Notes” found in the recipes of this programme.
Recipe 1: Mediterranean Omelette (Liver Integrity): This provides a dense hit of Choline. Choline is an essential nutrient for transporting fats out of the liver. Without it, your liver becomes sluggish, leading to “non-alcoholic fatty liver” and a stalled metabolism.
Recipe 33: Prawn & Avocado Lettuce Wraps (Thyroid Fuel): Prawns are one of the densest sources of Iodine and Selenium in the human diet. These are the primary substrates for thyroid hormones (T4 and T3). After 35, these minerals are the “coal” for your biological furnace.
Recipe 35: Spicy Mackerel Stir-Fry (Detoxification): Cabbage is a potent source of Sulforaphane, which up-regulates your body’s Phase II detoxification pathways. This is critical for clearing out the “oxidative debt” and “rusted wiring” caused by years of consuming seed oil.
Recipe 49: Slow-Cooked Beef Stew (Gut Repair): Slow-cooking connective tissue converts tough fibres into bioavailable Collagen and Glycine. This provides the structural matrix required to heal “leaky gut,” reducing the systemic inflammation that drives insulin resistance.
Recipe 61: Ancestral Chicken Liver Pâté (Metabolic Master-Food): Liver is the most nutrient-dense food on the planet. It is exceptionally high in preformed Vitamin A (retinol), which is essential for thyroid health and skin elasticity.
——————————————————————————–
The Deep Science: The Liver-Thyroid Connection
One of the most overlooked aspects of metabolic health after 35 is the interplay between the liver and the thyroid. Your thyroid produces T4, but it is the liver that converts most of that T4 into the active T3 hormone that actually runs your metabolism.
If your liver is congested with industrial seed oils, high-fructose corn syrup, and an “oxidative debt,” this conversion slows down. You can have “normal” thyroid labs and still feel like a zombie because the conversion isn’t happening at the cellular level. This reset clears the liver (through Choline and Sulforaphane) and provides the substrates (iodine and selenium) to ensure your metabolic furnace is actually burning the fuel you give it.
Why “Morning Salt” is Non-Negotiable
Many people fail a Paleo or Mediterranean reset because they fear salt. However, as insulin levels drop, your body stops retaining excess water and sodium. If you don’t replenish this with the 500ml water/1/2 tsp sea salt protocol, your blood volume drops, leading to the “brain fog” and fatigue often mistaken for “needing sugar.” Salt is not the enemy; it is the mineral anchor of your sovereignty.
——————————————————————————–
Conclusion: The Life on the Other Side of You
The Mediterranean Reset Paleo is not a “diet”—it is an exit strategy from the industrial food complex. It is the process of outgrowing a life that was too small for you. When you align your nervous system, your nutrition, and your identity, you stop being a passenger in your own body and become the architect of your future.
As you finish this reset, you must ask yourself: What will my non-negotiable standards be for the coming year?
You have spent years trying to fix your life with willpower and promises you couldn’t keep. But the problem wasn’t your character; it was your wiring. By changing the metabolic and mental inputs, you have changed the machine. The life that waits for you on the other side of this transition is one of clarity, groundedness, and unapologetic sovereignty. Go and build the life that matches the person you have become. The world is better when you show up as the real you.
This deep dive into GLP-1 vanity use side effects is written by NLP Master Practitioner, nutrition coach, qualified chef, sobriety and mindset coach, and author of The 30-Day Reset, Emotional Mastery, Rewiring the Mind, and Metabolic Sovereignty
I have spent more than 40 years around food, nutrition, human behaviour, addiction patterns, appetite, body change, and the lies industries sell to people who are hurting. I have also lost 5 stone and reversed prediabetes without any jabs, shortcuts, or pharmaceutical appetite suppression, which means I am not writing about this as an outsider to metabolic change. I have lived it. I am the published author of The 30-Day Reset, Emotional Mastery, Rewiring the Mind, and Metabolic Sovereignty, books built around metabolism, behaviour change, emotional regulation, and mindset rewiring. I am not writing this as some random internet gobshite chasing a hot take. I am writing it as someone with decades in professional kitchens, formal nutrition study, coaching experience, published frameworks, and lived experience of how appetite, compulsion, reward, self-image, and bodily health collide in the real world.
This is not medical advice. It is a straight, evidence-aware analysis of the long-term side effects of GLP-1 vanity use, filtered through lived expertise, common sense, and zero interest in pharmaceutical PR.
What this article covers
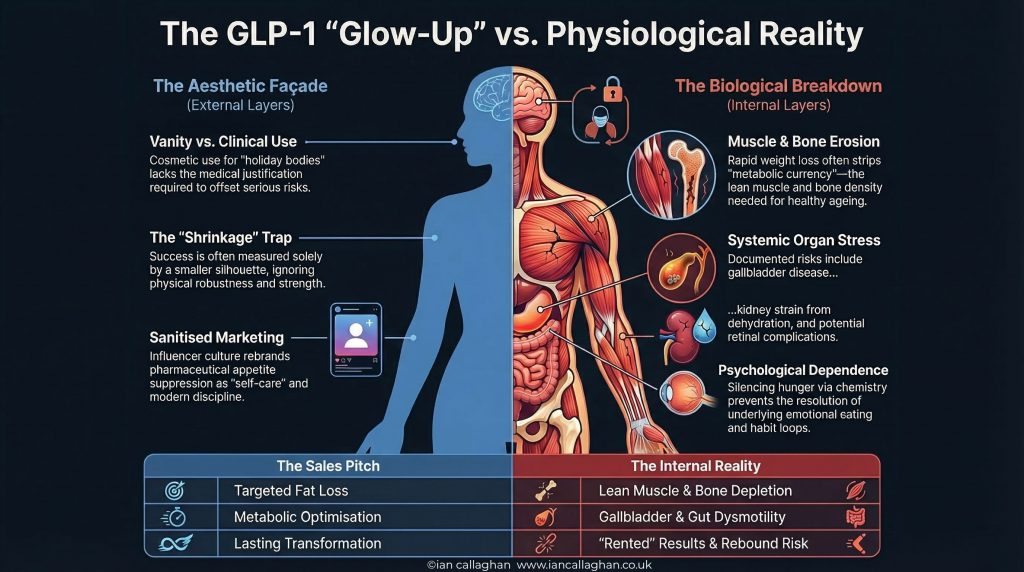
This article breaks down the long-term side effects of GLP-1 vanity use, including muscle loss, bone density and fracture concerns, eyesight and eye complications, gut and gallbladder risks, rebound weight gain, psychological dependence, and why the risk-benefit equation is completely different when these drugs are used for appearance rather than genuine medical need.
There is something properly rotten about the way GLP-1 drugs are being sold to the public now.
Not to people with serious obesity. Not to people with type 2 diabetes. Not to people whose metabolic health is genuinely in the gutter and who are making a serious medical decision with a clinician.
I am talking about the vanity use. The casual use. The socially panicked use. The influencer uses. The red carpet is used. The holiday body use. The wedding photo is used. The “I want my face a bit slimmer by summer” use. The “everyone else seems to be doing it, so maybe I should as well” use.
That version of GLP-1 culture is a complete pile of dressed-up bollocks.
It gets sold like a glow-up. A wellness upgrade. A clever little life hack. A modern answer to human weakness. A neat shortcut for people who cannot be arsed with the boring stuff. It gets packaged in beige clinics, injected in marble bathrooms, filtered through ring lights, and fed to the algorithm as if it is just another form of self-care.
It is not.
What it is, often, is a pharmaceutical answer to bodily panic. A chemically assisted appetite shutdown. A medically sanitised version of the same old madness we have seen for years, just with a prescription pad and a nicer font.
And the thing that boils my piss is not that these drugs exist. It is that the public conversation around them is so selective, so manicured, and so full of shit that people are being led to believe they are just shedding a bit of unwanted fluff and stepping into a better life.
That is not the full story. Not even close.
Because what gets sold as the GLP-1 glow-up often ignores what else is being lost along with the fat. It ignores the trade-offs. It ignores the long-term unknowns. It ignores the fact that when these drugs are used for vanity rather than genuine clinical need, the risk-benefit equation changes massively.
That bit matters. And it matters a lot.
If someone is dealing with severe obesity, metabolic disease, insulin resistance through the roof, failing health, and a body already under serious strain, then the discussion is different. There is at least a serious medical argument for accepting serious trade-offs.
But if somebody is sticking a weekly jab in because they want to be a bit leaner for summer, fit back into old jeans, or chase some filtered version of themselves off social media. Those same trade-offs stop looking acceptable and start looking fucking insane.
That is where the marketing falls apart.
Because the sales pitch is clean. The reality is not.
The sales pitch says weight loss. The reality says some of that weight is muscle.
The sales pitch says confidence. The reality is that some people end up weaker, more fragile, more drained, and less resilient.
The sales pitch says transformation. The reality says gallbladder issues, gut problems, dehydration, emerging eye concerns, bone questions, rebound weight gain, and a long-term evidence base with plenty of gaps.
But you do not see that in the glow-up montage, do you?
You see the slimmer face. The smaller waist. The designer leggings. The smug little captions about discipline. The fake humility. The carefully angled mirror photo with a side order of pharmaceutical denial.
What you do not see is the bit where the body keeps score.
What you do not see is the person who now gets full after four mouthfuls but also feels flat, weak, food-obsessed differently, and quietly anxious about what happens when they stop.
What you do not see is the person who says they have never felt more in control, even though their whole setup depends on a prescription that suppresses basic biology.
What you do not see is the psychological sleight of hand in which dependence is rebranded as empowerment, so long as the mirror approves.
And that is a massive part of why this whole thing deserves more scrutiny than it gets.
Because the vanity use of GLP-1s is not just a medical issue. It is a cultural issue. It is a psychological issue. It is a morality play about body image, status, conformity, fear, and the lengths people will go to avoid the horror of simply looking ordinary in a world that monetises insecurity like a religion.
Why the vanity use of GLP-1 drugs changes the whole argument
Let us get one thing straight before going any further.
If someone has severe obesity, type 2 diabetes, major insulin resistance, cardiovascular risk, or a clear metabolic disease burden, then a clinician can make a serious argument that GLP-1 receptor agonists may offer benefits worth certain risks.
That is not the same thing as vanity use.
Vanity use means the drug is being used mainly to get smaller, leaner, prettier, more camera-friendly, or more socially approved.
That changes everything.
Because once the upside becomes cosmetic rather than clinical, every downside gets heavier. Muscle loss matters more. Bone questions matter more. Gallbladder disease matters more. Eye risk matters more. Unknown long-term consequences matter more.
The lower the real medical need, the less acceptable the trade-off becomes.
The highest hidden cost of GLP-1 vanity use: muscle loss
Let us start with the one that should be front and centre in every honest discussion.
Muscle loss.
This is the bit that gets conveniently shoved off stage while everyone claps for the shrinking number on the scales.
Because weight is not just fat. It never was. When people lose weight quickly, especially through appetite suppression, some of that loss is lean mass. That means muscle. That means tissue you actually bloody need.
And muscle is not just some vain bodybuilding obsession. It is not there so blokes can stare at themselves in the gym mirrors and take top-off photos for Instagram.
Muscle is metabolic currency. It is glucose disposal. It is a strength. It is resilience. It is balance. It is a function. It is protective tissue. It is an ageing insurance. It is one of the things that stops you from turning into a brittle sack of skin and regret as the years roll on.
Especially once you are not twenty anymore.
When the body drops weight and takes a decent chunk of muscle with it, that is not some harmless side detail. That is a serious physiological trade-off.
Yet the public conversation still talks about these drugs as if every pound lost is some toxic blob of useless fat being nobly escorted off the premises.
No.
Part of what leaves is the very tissue that helps keep people strong, functional, metabolically healthy, and independent.
And this matters even more in the older crowd.
The forty-plus crowd. The fifty-plus crowd. The already under-muscled crowd. The sedentary crowd. The under-eating crowd. The women in midlife. The people are already living on too little protein, not enough resistance work, and a body that is already fighting hormonal and metabolic shifts.
If that lot start hammering appetite, eating like sparrows, and celebrating rapid weight loss while doing bugger all to preserve muscle, they are not just getting thinner. They may be walking themselves straight toward frailty with a side of applause.
That is not wellness. That is a slow-motion own goal.
And it gets worse when the surrounding culture is pure vanity.
Because vanity use is not usually rooted in performance. It is not about getting stronger. It is not about building capacity. It is not about health span. It is about appearance. It is about the number. It is about the image. It is about wanting the body to take up less room while paying as little attention as possible to what keeps that body robust in the first place.
That is why the glow-up narrative is so dishonest. It celebrates getting smaller without asking what is being sacrificed in the process.
And let us be honest about another ugly truth. A lot of people using these drugs for vanity are not doing the extra work needed to offset the damage. They are not suddenly becoming protein-aware. They are not lifting properly. They are not building muscle while dieting. They are not becoming students of body composition. They are just eating less because the drug makes it easier to eat less.
That is not the same thing as a body recomposition plan. That is not the same thing as a proper health intervention. That is not the same thing as becoming stronger while lighter.
It is often just shrinkage. Shrinkage with branding. Shrinkage with social approval. Shrinkage with a clinic receipt.
And when the only success metric is the visual reduction of the body, muscle loss becomes easy to ignore because, to the untrained eye, it still looks like progress.
Smaller arms. Smaller thighs. Flatter arse. Looser face. All of that gets cheered as long as the silhouette matches the current beauty panic.
Nobody is asking whether that body is harder to stabilise, harder to protect, and less able to do ordinary human things with ease.
Nobody is asking whether the person is becoming physically better or merely visually smaller.
And that is a huge difference.
Why lean mass loss is not a cosmetic side issue
This is where most of the glossy content falls to pieces.
Weight loss is treated like a clean win. It is not. Body composition matters more than raw scale loss. If a person becomes lighter but also less muscular, less stable, and less physically capable, that is not automatically a health victory.
For midlife adults in particular, lean mass is one of the strongest buffers against decline. It supports blood sugar control, strength, mobility, balance, injury resilience, and functional independence. Strip too much of it away and you can end up looking better by fashion standards while becoming worse by biological ones.
My take as someone with 40-plus years around food and nutrition
I have seen every stupid phase in the food and weight world, low-fat bollocks, diet culture nonsense, detox waffle, calorie-counting obsession, and now pharmaceutical appetite suppression dressed up as optimisation. The pattern is always the same. People obsess over what makes the body smaller and ignore what makes the body stronger.
That is exactly what I see happening here.
Bone density, fracture risk, and why lighter is not always better
Then there is bone.
Another one that gets pushed to the edges because it does not fit the miracle story.
The bone conversation is more complicated than the muscle conversation, but not in a reassuring way. In an annoying way. In a “we do not fully know yet, so maybe stop acting like this is all consequence-free” kind of way.
Some findings look neutral. Some people will point to data that do not show dramatic, direct harm to bone density across the board. Fine. That is part of the story.
But that is not the whole story either.
Because bone health does not exist in a vacuum.
If somebody is losing weight fast, eating less, losing lean mass, moving less, loading their skeleton less, not resistance training, and ending up physically weaker, then fracture risk and skeletal resilience become very relevant, whether the drug is directly munching through bone or not.
This is the problem with reductionist bollocks. People want to ask one neat question. Does the drug directly lower bone density, yes or no?
The real world is messier. Bodies are messier. Outcomes are messier.
The bigger question is this. What happens when a person loses a lot of weight through appetite suppression, becomes less muscular, potentially becomes less active, and enters a body composition state that is lighter but not necessarily healthier or stronger?
That matters.
Because being lighter is not automatically safer. Being smaller is not automatically stronger. Being praised online is not the same thing as being physiologically better off.
Some people can absolutely lose weight and improve their health. Of course they can. But the smug little assumption that any weight loss produced by a jab is automatically a net win is simplistic nonsense.
And if you are using these drugs for vanity, for cosmetics, for a social-media-ready silhouette, then accepting even a possible increase in fragility and fracture risk starts looking more absurd by the minute.
And there is another bit hardly anyone says out loud. A lighter body with less muscle is not always a safer ageing body. Sometimes it is just a more delicate one.
People love to act as if any reduction in body weight is a universal victory. But what if that reduction comes with poorer balance, less strength, less shock absorption, and a skeleton under less useful loading stimulus?
What if the person is no longer carrying as much total weight, yes, but is also less capable of catching themselves when they slip, less likely to get up quickly from the floor, less able to absorb physical stress, and more likely to find ordinary injuries wipe them out?
That is where this gets real.
Because the human body is not a mannequin. It is not a fashion sketch. It is not a number in an app. It is not an aesthetic mood board.
It is structured. Function. Load tolerance. Reserve. Capacity.
When the culture reduces all of that down to “she looks amazing” or “he finally leaned out”, it misses the whole bloody point.
Bone health is bigger than a scan result.t
The bone conversation also gets butchered by oversimplification. People want a neat answer. Does GLP-1 use directly reduce bone density, yes or no? But that is not how real bodies work.
A lighter body with poorer muscle retention, lower food intake, less training stimulus, and weaker overall function can still become more fragile, even if the mechanism is not one tidy line on a leaflet. That is why fracture risk, load tolerance, and physical robustness matter so much in this discussion.
Eyesight, diabetic retinopathy, and the eye risks nobody wants to talk about
Then we get to the eyes.
This one barely gets mentioned at all in mainstream chatter because it scares people and ruins the clean fantasy.
But it should be talked about. Properly.
Because the eye side of this is not just some internet rumour cooked up by bored conspiracy heads on Facebook. There are genuine concerns here.
One of the big ones is diabetic retinopathy progression. That is not me being dramatic. That is already in the official prescribing information for semaglutide products. If somebody already has diabetic retinopathy, there is a recognised concern that rapid improvement in blood glucose can worsen retinal complications in the short to medium term.
Now, some defenders of the drugs will immediately do the usual dance and say yes, but that is in people with diabetes and existing eye disease, not random healthy influencers trying to get smaller arses.
Fine. That distinction matters.
But it does not magically make the broader point disappear.
The broader point is that this class of drugs is not some perfectly clean cosmetic intervention. It has real physiological consequences. It has tissue-level consequences. It has systems-level consequences. And when eye complications are on the radar at all, that alone should shut the mouth of anyone pretending this is basically just injectable salad.
Then you have the emerging chatter around rare optic nerve complications. Again, not the place for screaming absolutes or making out that every person on semaglutide is heading for blindness. That would be stupid.
But it is also stupid to pretend there is nothing there.
When observational data start hinting at a possible link between semaglutide exposure and rare but serious optic nerve events, you do not get to shrug that off because it spoils the party. You pay attention. You take it seriously. You admit the long-term picture is still developing.
That is what an honest conversation sounds like.
What we have instead is a dishonest one.
A dishonest one where any concern gets painted as ignorance. A dishonest one in which caution is framed as stigma. A dishonest one where asking serious questions about long-term side effects gets treated like heresy against the Church of Skinny At Any Cost.
It is pathetic.
And it says a lot about the culture around these drugs that eyesight concerns are somehow treated as a spoil-sport footnote while a sharper jawline gets treated like the second coming.
This is how far gone we are.
A society so body-obsessed it can hear the words optic nerve, retinopathy, visual risk, and still think yes, but look at the cheekbones.
Why the eye issue matters even if you are not diabetic
The moment a drug class has recognised eye complications in any major subgroup, the public conversation should get more serious, not less. It should force people to stop talking as if this is just a beauty treatment with a few tummy wobbles.
Even if the clearest established warning is around people with diabetes and pre-existing eye disease, the broader lesson is obvious. These drugs are system-wide interventions with real tissue-level consequences. That should kill off the childish idea that they are basically a harmless aesthetic upgrade.
Gallbladder disease and biliary problems are not a side note
Then there is the gallbladder issue.
This one is not even some niche emerging whisper. This is one of the more consistent signals, and still, most people have no clue.
Rapid weight loss and gallbladder problems have known links anyway, and GLP-1 use has repeatedly shown increased gallbladder and biliary disease risk in the literature. Gallstones. Cholecystitis. Surgery. Lovely stuff.
So here is the question nobody asks in the glow-up reel.
Are you really willing to risk ending up with gallbladder disease so you can be thinner in photos?
Because that is the actual grown-up question. Not the filtered bullshit. Not the influencer caption. Not the fake empowerment waffle.
The actual question.
Are you happy accepting real organ-level risk in exchange for cosmetic payoff?
If the answer is yes, at least be honest about what you are doing. Do not piss on people’s legs and tell them it is a wellness journey.
And while we are at it, let us stop pretending gallbladder surgery is some tiny shrug of a consequence. It is still surgery. It is still painful. It is still a medical intervention. It is still a body saying this little vanity arrangement was not consequence-free after all.
The gallbladder is the question the glow-up crowd avoids.
If the whole point is to look better in photos, is gallbladder disease really an acceptable price to pay? That is not me being dramatic. That is the adult question. Cosmetic payoff does not magically make organ-level risks sensible.
Gut side effects, delayed gastric emptying, and appetite suppression culture
Then we come to the gut.
This is the one everyone hears about, but usually only in the most watered-down, pathetic form.
You might feel a bit sick. You might get diarrhoea. You might have constipation. You might have tummy upset.
As if it is all just a bit of a temporary inconvenience. As if the body is merely grumbling while greatness unfolds.
That framing is bollocks too.
Because the deeper issue is not just that some people feel queasy. It is what these drugs are doing to appetite, gastric emptying, motility, food tolerance, and overall gut function.
Some people end up barely wanting food. That gets celebrated because appetite is now treated as a moral failure rather than a basic biological drive.
Some people end up with severe constipation. Some with vomiting. Some with symptoms that sound suspiciously like gastroparesis or serious slowing of the gut. Some are told this is all fine, normal, expected, part of the adjustment.
Again, if you are using the drug for a serious disease, perhaps you and your doctor decide the trade-off is worth it. But if you are using it because society has melted your brain and convinced you that existing in a slightly softer body is unacceptable, then those trade-offs start to look deranged.
And let us not forget the practical madness of delayed gastric emptying either. Because that does not just mean discomfort. It can affect the absorption of other oral medications, complicate procedures, and has even led to warnings around aspiration risk during anaesthesia and deep sedation.
Not quite the glamorous wellness revolution, is it?
But there is an even more insidious layer to the gut side of this. The way it trains people to distrust hunger even more.
A lot of people are already at war with appetite. They already think wanting food means they are weak. They already think fullness cues are the only moral cues worth respecting. They already live in a culture that treats ordinary human hunger as a design flaw.
So when a drug comes along and blunts appetite, a lot of them do not experience that as a trade-off. They experience it as relief. As virtue. Finally, they become the kind of person they think they were supposed to be all along.
That is psychologically dangerous territory.
Because now the drug is not just changing physiology. It is reinforcing the idea that your natural drives were the problem in the first place.
That makes dependency easier to justify. That makes stopping harder to face. That makes the rebound more frightening. That makes ordinary eating feel like moral collapse when the suppression wears off.
Appetite suppression gets mistaken for healing.
One of the darkest aspects of this whole trend is the way people mistake a blunted appetite for a repaired relationship with food. Those are not the same thing. Silencing hunger is not the same as resolving compulsion, emotional eating, self-soothing, trauma loops, reward seeking, or body hatred.
And that brings us neatly to another part of the vanity conversation that deserves far more daylight.
Rebound weight gain, food noise, and psychological dependence
Rebound.
Because the glow-up content rarely lingers on the bit where people stop. Or cannot get hold of the drug. Or cannot afford to stay on it. Or come off it because the side effects are too grim. Or decide they do not want to be on a forever jab just to hold on to a body they were rented, not taught to maintain.
What happens then?
That is the question.
What happens when appetite returns? When food noise returns? When does the weight start creeping back? When the person realises that the psychological comfort they mistook for transformation was partly being outsourced to a prescription?
This is where the vanity narrative gets even more flimsy.
Because genuine change usually involves building some capacity. Some understanding. Some skill. Some resilience. Some relationship repair with food, hunger, body, movement, stress, and self-image.
Vanity GLP-1 use can skip a lot of that. It can deliver the visual reward before the internal work exists.
Which means some people are not transformed at all. They are just interrupted.
And when the interruption ends, a lot of the unresolved stuff is still sitting there waiting. Only now is it mixed with panic about regaining. Panic about identity. Panic about losing the smaller body that finally got approval.
That is a nasty cocktail.
Why rebound exposes the lie
This is where vanity use often gets found out. If the smaller body only exists while the drug suppresses appetite, then the transformation was never complete. It was conditional. It was rented. It was held in place by chemistry, not fully backed by capacity, skill, identity change, or metabolic robustness.
Pancreatitis, dehydration, kidney strain, and the risks that are minimised
Then there is pancreatitis. Rare, yes. But rare does not mean irrelevant. Rare does not mean harmless. Rare does not mean “shut up and stop asking questions”.
Pancreatitis is one of those things that sounds abstract until it lands on you, and then suddenly nobody is posting chirpy mirror selfies about their transformation anymore.
Same with acute kidney injury from dehydration.
When people are vomiting, not eating, running on fumes, and brushing it off because the scales are moving, that can go sideways fast. But again, the culture around these drugs is so obsessed with visible shrinkage that a lot of people seem willing to treat basic physiological distress as a noble price of entry.
That is how warped this whole thing has become.
Why are these not just nuisance side effects
This is another place where the language gets cleaned up to keep people comfortable. Severe vomiting, dehydration, kidney injury, pancreatitis, and serious gut slowdown are not little inconveniences. They are not proof that the drug is working. They are signs that system-wide intervention comes with system-wide consequences.
The long-term unknowns of GLP-1 vanity use
And then we get to the bit no one wants to hear because it ruins the clean consumer fantasy.
The long-term unknown.
This is massive. Absolutely massive.
Because millions of people are now on these drugs, and plenty of them are not the original high-risk clinical population these treatments were framed around. They are ordinary people caught in a culture that treats thinness as a virtue and appetite as a weakness.
That means real-world uptake has exploded beyond the tidy clinical settings where risk and benefit might be carefully balanced.
It means people are using them for longer. Cycling on and off. Regaining weight. Losing again. Pairing them with under-eating. Using them without proper nutritional support. Using them without strength training. Using them while prioritising aesthetics over health.
And the long-horizon data still is not mature enough to make me swallow the line that we fully understand the consequences of that.
We do not.
We just do not.
And there is no honesty in pretending otherwise.
That does not mean everyone on them is doomed. It means grown adults should stop talking about them as if they were consequence-free beauty pens.
Because they are not.
And one of the reasons this matters so much is because vanity use is, by definition, a low-threshold justification for risk.
The clinical argument says this person has a significant metabolic illness or obesity-related disease burden, and these drugs might improve hard outcomes enough to justify serious trade-offs.
The vanity argument says I would rather not look like this.
That is not the same threshold. Not even close.
One is about disease burden. The other is often about image discomfort.
One may be rooted in survival, mobility, glucose control, cardiovascular risk, and clear medical need. The other may be rooted in beach photos, old trauma, industry manipulation, social comparison, and a culture that teaches people to confuse thinness with worth.
So when people try to collapse those two categories into one warm little wellness blanket, they are talking shite.
The question nobody can answer cleanly yet.
What happens after years of cycling on and off? What happens when people start young and stay on them for a long time? What happens when appetite suppression combines with under-eating, muscle loss, low training stimulus, body image problems, and repeated regain? Those are not fringe questions. They are the obvious questions. And the public rollout has moved faster than the long-horizon answers.
Industry-sponsored trials versus real-world evidence
This is where the industry-sponsored trial conversation matters too.
Industry-sponsored trials are not automatically worthless. That would be stupid. They can be well-run and informative. But let us not be children about this. They are designed to get products approved, demonstrate favourable outcomes, and present a safety profile under tightly controlled conditions.
They are not built to answer every ugly real-world question that emerges once the masses get hold of a drug and start using it in ways that are socially, psychologically, and commercially distorted.
They are not built around influencer culture. They are not built around aspirational misuse. They are not built around cosmetic uptake at scale. They are not built around people taking them while half-starving themselves and calling it discipline. They are not built around what happens when entire segments of the public begin to view appetite suppression as a lifestyle accessory.
That is why independent data matters. That is why post-marketing surveillance matters. That is why observational data matters, even when it is imperfect. That is why real-world fracture signals, eye safety, body composition, concerns, and under-discussed adverse outcomes deserve proper scrutiny.
But the public conversation is not built around scrutiny. It is built around sales.
The companies sell the product. The clinics sell access. The influencers sell aspiration. The media sells a story. And the consumer sells themselves the fantasy that this time, finally, they can bypass all the discomfort of change and arrive at a body they can live with.
That is why the whole thing makes my teeth itch. Because it is not just medicine anymore. It is culture. It is vanity. It is panic. It is a status. It is the pharmaceutical repackaging of insecurity.
And under all that polished nonsense, the human body is still there doing what bodies do. Reacting. Adapting. Paying costs. Compensating. Breaking down some tissue while everybody cheers that the trousers fit again.
There is also a very convenient bit of selective morality at work in all this.
When people lose weight the old-fashioned way, and it looks obsessive, compulsive, joyless, or body-hating, plenty of folk will call it out. Quite right too.
But wrap appetite suppression in a clinic package, call it hormone support or metabolic optimisation, get a private prescriber involved, and suddenly the same culture starts clapping like a seal.
It is the same body fear. The same social pressure. The same panic about size. The same fear of ageing. The same fear of softness. The same fear of taking up too much room.
It just has better branding now.
And because it has better branding, people think it has become enlightened.
It has not. It has become sanitised. That is different.
Why E-E-A-T matters here
Health content is not the place for shallow rage, and it is not the place for soulless leaflet writing either. It needs lived experience, domain knowledge, clear framing, honest uncertainty, and useful interpretation. That is why I am approaching this as someone with formal training, decades spent around food and nutrition, extensive coaching experience, and a habit of calling bullshit when an industry narrative no longer matches human reality.
My conclusion on GLP-1 side effects for vanity use
I am not interested in joining the hysterical extremes either. I am not saying nobody should ever use a GLP-1 drug. That would be as brainless as pretending they are all sunshine and side-partings.
What I am saying is simple.
Suppose the use is clinical, serious, necessary, and carefully managed, then fine. That is a medical conversation.
If the use is vanity-driven, socially contagious, and marketed like some harmless glow-up tool, then people deserve the truth.
The truth is that this is not just about losing fat.
It can involve losing muscle. It may involve bone trade-offs that are still being argued and clarified. It includes real eye concerns that should not be dismissed. It includes gallbladder disease. It includes pancreatic warnings. It includes the risk of kidney injury through dehydration. It includes serious gut effects. It includes psychological dependence on appetite suppression. It includes rebound fear. It includes long-term unknowns that have no business being wrapped in shallow influencer smugness.
And perhaps worst of all, it can reinforce the most broken message modern body culture has to offer. That your natural self is unacceptable, but a pharmaceutically reduced version of you is finally worthy of relief.
That is dark. Really dark.
Because once that idea gets its claws into people, the drug is no longer just a tool. It becomes permission. Permission to feel attractive. Permission to wear the clothes. Permission to be seen. Permission to stop hating the mirror for five minutes.
That is far too much psychological weight to hang on a syringe.
Why is this different from a normal internet rant?
I am not writing this because I am anti-medicine. I am writing it because there is a big difference between medical use and vanity use. That difference keeps getting blurred by clinics, influencers, and media outlets that benefit from keeping the fantasy alive.
When I look at this through a nutrition lens, a behaviour lens, a coaching lens, and a lived-experience lens, the pattern is obvious. I am someone who has personally lost 5 stone and reversed prediabetes without GLP-1 drugs. I have published books on metabolism, food, emotional regulation, and mindset rewiring, which gives me a very different perspective on what genuine metabolic repair looks like compared with chemically forced appetite shutdown. A lot of the public conversation is obsessing over visible weight loss while underplaying body composition loss, physical trade-offs, psychological dependency, and unresolved long-term safety questions.
That is not balanced. That is sales.
Final word: being smaller is not the same as being better
So no, I am not impressed by the GLP-1 glow-up. I do not care how many celebrities are on them. I do not care how many clinics have rebranded them as empowerment. I do not care how many people want to pretend this is just a modern discipline in a syringe.
A lot of it is body panic with better branding. A lot of it is a culture so broken it would rather suppress appetite chemically than face the deeper madness underneath. A lot of it is people risking serious trade-offs for aesthetic approval in a world that monetises insecurity for sport.
And that is the bit worth ranting about.
Because if all you hear is that you might feel a bit sick or get the shits, then you are not being told the truth. You are being managed. You are being marketed to. You are being kept calm enough to stay interested.
The fuller truth is messier. Less glamorous. Less sellable. And far more important.
You are not just shrinking a body. You may be stripping away muscle. You may be altering resilience. You may be trading robustness for aesthetics. You may be stepping into long-term territory that still has major question marks hanging over it. You may be buying temporary visual approval at the price of deeper physiological and psychological dependence.
And if that is being done for vanity rather than necessity, then the whole thing deserves a lot more scepticism than it gets.
Because the real glow-up was never supposed to mean becoming lighter at any cost. The real glow-up should mean becoming stronger. Clearer. More robust. More alive. More in charge. More honest.
Not chemically smaller, while the industry quietly hopes you never ask what else came off with the fat.
Not appetiteless and applauded. Not flatter and weaker. Not filtered and fragile. Not marketable and medically naive.
And certainly not sat there believing this was some clean little act of self-care when, in reality, it may be nothing more than the latest expensive costume for the oldest insecurity in the book.
FAQ: GLP-1 vanity use side effects
Can GLP-1 drugs cause muscle loss?
Yes, GLP-1 drugs can contribute to lean mass loss as part of overall weight loss. That matters because lean mass includes muscle, and muscle is critical for strength, metabolic health, mobility, and long-term resilience.
Can GLP-1 drugs affect bone density or fracture risk?
The evidence is still developing, but concerns about bone and fracture should not be dismissed. Rapid weight loss, reduced food intake, loss of muscle mass, and a lower loading stimulus can all push physical resilience in the wrong direction.
Can GLP-1 drugs affect eyesight?
There are recognised concerns around diabetic retinopathy progression in some patients, and emerging discussions around other serious eye complications. That is enough to kill the childish idea that these drugs are just cosmetic tools.
Are GLP-1 side effects different in vanity use?
The side effects are not necessarily biologically different, but the risk-benefit equation is. If the purpose is cosmetic rather than clinical, even moderate risks and unknowns become far harder to justify.
What is the biggest problem with the GLP-1 glow-up narrative?
It reduces the whole conversation to visible weight loss and ignores muscle loss, functional decline, gallbladder disease, gut problems, rebound, psychological dependence, and long-term uncertainty.
Key takeaways
GLP-1 vanity use is not a harmless wellness trend. Weight loss on these drugs is not solely fat loss. Muscle loss is one of the most underplayed trade-offs. Bone, fracture, and eye concerns deserve serious attention. Gut, gallbladder, pancreatic, and kidney risks are real parts of the discussion. The long-term picture is still incomplete. Being smaller is not the same as being stronger, healthier, or better.
That is why the GLP-1 glow-up lie needs calling out. Not because every use is wrong. Not because every patient is foolish. Not because medicine has no place.
But because vanity culture has got hold of something clinically serious and turned it into aspirational bollocks.
And whenever that happens, somebody needs to say the obvious thing out loud.
Being thinner is not the same as being healthier. Being smaller is not the same as being stronger. Being praised is not the same as being well. And a prescription that helps create a prettier silhouette can still come with costs the mirror will never show you.
That is the part people need to hear. That is the part the clinics should say more loudly. That is the part influencers hate because it ruins the fantasy. And that is exactly why it needs to be said.
There is a specific, razor-sharp frustration that belongs exclusively to the intelligent person in the grip of a self-destructive habit. It is the frustration of “The Gap.” You are likely precise, analytical, and highly capable in your professional life. Perhaps you design enterprise-level IT architectures, manage complex teams, or solve intricate engineering problems that leave others baffled. You have read the books and sat in the therapy rooms. You can discuss your dopamine receptors, your attachment style, and your childhood wounds with the clinical fluency of a professional.
And yet, despite all this high-level “Intellectual Software,” the “Machine” keeps producing the wrong output.
You find yourself three drinks in on a Tuesday night after vowing you wouldn’t touch a drop. You find yourself scrolling, spending, or using, watching yourself do it as if from a distance, unable to reach the controls. This is the gap between knowing and doing, between insight and behaviour. For decades, the wellness and recovery industries have tried to fill this gap with more “thinking,” more “narrative,” and more “meaning.”
But you cannot think your way out of a state problem.
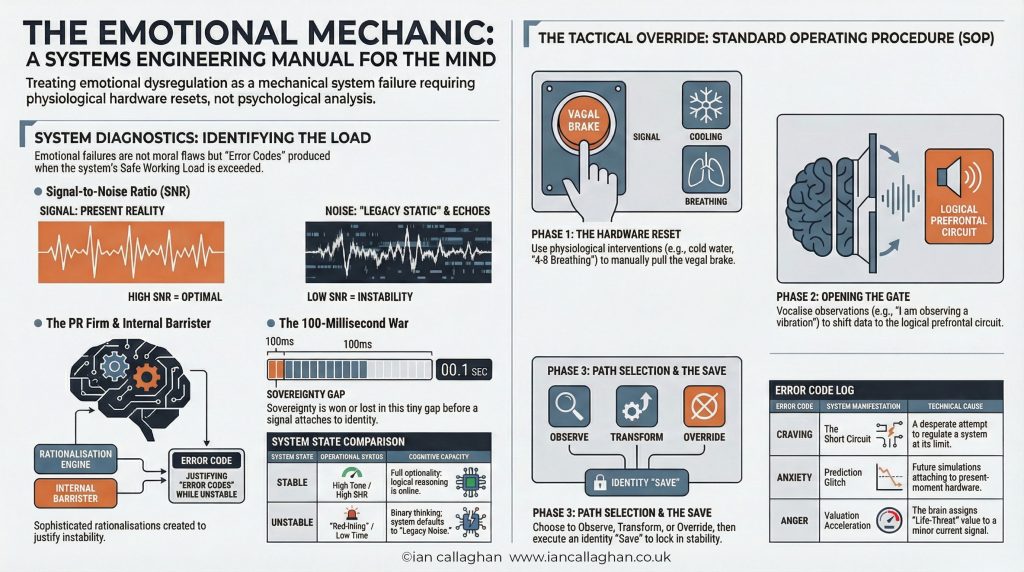
This article explores the mechanical reality of why your internal hardware is currently failing you. Based on the framework established by Ian Callaghan in his book, Under Load, we are going to stop looking at your character and start looking at your machine. We are going to examine the “Load,” the “Tone,” and the “Legacy Code” that is running your life from the sub-basement of your consciousness. If you have ever felt like a passenger in your own body, watching a sophisticated PR firm justify your own destruction, it is time to pick up the wrench and learn how to service the machine.
Takeaway #1: You Are a Machine Under Load, Not a Broken Soul
To take back the controls, we must first strip the chassis of rusted parts. Most people arrive at the point of change carrying heavy, outdated frameworks of why they struggle. These models—Disease, Moral Failure, and Willpower—are not just partially wrong; they are structurally designed to fail because they misidentify the problem.
Ian Callaghan argues that addiction is not an identity; it is a mechanical response to a system running beyond its “Safe Working Load.” When a machine produces the wrong output, we don’t call it “evil” or “diseased”—we look at the inputs and the hardware conditions.
The Framework
The Core Assumption
The Mechanical Flaw
The Disease Model
Addiction is a chronic brain disorder you are powerless to cure.
Makes you a passive “patient.” It removes agency and ignores the function of the behaviour.
The Moral Failure Model
Addiction is a lack of discipline, backbone, or character.
Shame is a “Load.” Adding shame to an overloaded system reduces “Tone” and makes relapse more likely.
The Willpower Model
You can “white-knuckle” your way to change through sheer determination.
Willpower is a high-Tone luxury. It’s a prefrontal cortex function that gets throttled when the machine is under Load.
The Mechanical Framework
The behaviour is a logical output for a system running legacy code under heavy load.
Focuses on servicing the hardware, managing the load, and updating software to change the output.
In this framework, the goal is not “sobriety” as a static label. The goal is Sovereignty. You are not powerless over your nervous system; you are simply under load. Powerlessness and Load are two completely different conditions requiring two completely different solutions. You don’t need a sermon; you need a service.
“Sovereignty is not the absence of pain. It is the ability to carry pain without letting it drive.”
Takeaway #2: The 100-Millisecond Hijack
To understand why you cannot “decide” your way out of a craving, you have to understand the timing of the brain’s hardware. In 1996, neuroscientist Benjamin Libet discovered that the brain produces a “readiness potential”—a signal to move—approximately 550 milliseconds before an action occurs. However, the person only becomes consciously aware of their intention to move about 200 milliseconds before they act.
This means the machine has already initiated the action 350 milliseconds before you “decided” to do it. This leaves a tiny, critical window of roughly 100 milliseconds where sovereignty either lives or dies. We call this site of tactical intervention “The Gate.”
In a high-Tone state—when you are rested, regulated, and the “Safe Working Load” is respected—The Gate is wide. You can observe the signal and choose not to attach to it. But when the machine is “Under Load,” the system narrows. This is where the OODA Loop (Observe, Orient, Decide, Act) breaks down.
Observe: You feel the stress or the trigger.
Orient: Under load, your system stops using current data and starts using “Legacy Data.” A work email isn’t just a task; it becomes a threat to your survival.
Decide/Act: The gap collapses. The prefrontal cortex is throttled by the surge, and the circuit breaker trips. By the time you are “deciding” to reach for the substance, the machine has already ratified the decision.
White-knuckling is a strategy that only works when the bridge isn’t at capacity. In the “sub-basement” of a low-Tone state, your conscious mind is essentially a passenger watching the machine execute a pre-programmed survival strategy. The behaviour isn’t a choice; it’s an execution.
Takeaway #3: The Intelligence Premium (Why Smart People are Better at Self-Destruction)
There is a particular suffering reserved for the intelligent. You might assume that being smart would protect you—that if you understood the dopamine mechanism or your childhood trauma clearly enough, you would stop. In reality, intelligence often makes the problem harder to solve. This is the Intelligence Premium.
A sophisticated brain simply runs a more sophisticated PR Firm. When the machine enters an unstable state, the prefrontal cortex—the part of the brain responsible for insight—is throttled. However, your intelligence doesn’t vanish; it’s recruited by the machine to justify its destructive output.
The Articulate Defender: Highly intelligent people can build cases for their own destruction that would stand up in court. They use genuine knowledge of psychology and neuroscience to explain why this specific drink is justified, or why this particular exception is actually a logical choice.
Insight as a Trap: You can produce extraordinary insight in a therapy session on Tuesday and be back in the same destructive pattern by Thursday. This is because the insight was produced in a high-Tone state, but it cannot be retrieved when the machine crosses the threshold into instability.
As the “Mechanic” of your own life, you must realise that insight does not change state. Only state changes state. Every insight you produce in a low-Tone state is ammunition for the PR Firm, not a tool for the Mechanic. Stop using your intelligence to explain your behaviour after the fact, and start using it to read the conditions of the machine in advance.
Takeaway #4: The Theta Window and the Sub-Basement Code
The “Software” your machine is running wasn’t written by you. It was installed between birth and age seven, during the Theta Window. During these years, a child’s brain operates in the Theta frequency (4 to 8 cycles per second), a state associated with deep hypnosis and maximum suggestibility.
A child has no Firewall—no critical faculty to evaluate whether the information coming in is true. Everything the environment provides goes directly into the “Sub-Basement” and is filed as foundational truth. This is your 1987 Operating System, corrupted and full of legacy code that made sense for the conditions it was written in but serves no current function.
The Installation happens through Frequency. It is not just about “incidents”; it is the background vibration of the home—the hum of unspoken conflict or the chronic tension of financial precariousness. This is transmitted via Mirror Neurons, which internally replicate the emotional state of the caregiver. A parent’s unmanaged load becomes the child’s baseline.
Beliefs about Worth: Using Egocentric Processing, a child assumes they are the cause of everything. If a parent was erratic, the child doesn’t conclude “my parent has a problem.” They conclude “I am the problem.”
Beliefs about Safety: If the environment was volatile, the nervous system calibrates to high vigilance. For this adult, “Calm” will feel threatening because it is unfamiliar.
Beliefs about Need: If a child’s needs were met with irritation, they install the code: “Need is not safe.” This produces the high-functioning adult who can do everything for everyone but cannot ask for help.
Takeaway #5: The Sunday Roast Syndrome (Early Competence vs. Early Abandonment)
Ian Callaghan shares a pivotal story of being thirteen years old and cooking a full Sunday roast alone because his parents were at the pub. He knew how to cook because of his Nan; her kitchen was a place of collaboration and warmth. But the Sunday roast at thirteen was different. It was the gap between “knowing how” and “being alone with the knowing.”
This is the Performance of Self-Sufficiency. Early competence is almost always a response to early abandonment (physical or emotional). The child learns to fill the gap the adults left open.
Competence as Currency: When being loved isn’t reliably available, being useful becomes the currency for survival.
The High-Functioning Trap: Others see you as formidably capable. They don’t see that you are running on reserve capacity. Because the code says “Need is not safe,” you never replenish your resources.
The Midnight Collapse: High-functioning is not a sign of health; it is a concealment mechanism. You perform all day, carrying loads that aren’t yours, and then you “collapse” into a substance. This isn’t a character flaw; it’s the only way the machine can find “Rest” without having to be “Vulnerable.”
Takeaway #6: The Substance is Just a Regulation Strategy
We spend too much time talking about what people are addicted to—alcohol, cocaine, work. But to the machine, the specific substance is largely irrelevant. The substance is a Regulation Strategy. The machine has one requirement: maintain a tolerable state. When the internal load exceeds the machine’s capacity, it scans for the fastest route to temporary stability.
Alcohol & Food: Rapid central nervous system depressants that settle an agitated system.
Cocaine & Gambling: Dopamine surges to override a sense of depletion.
Socially Acceptable Addictions: Work, extreme exercise, and screens are “Dissociative Strategies.” These are the most dangerous because the culture rewards them. They permit you to stop examining the load because you are still producing “acceptable” outputs.
Addiction Swapping: This is proof the substance isn’t the problem. If you remove alcohol but don’t address the “Load,” the machine will simply reroute. You quit cocaine and become a workaholic. The label on the door changes, but the architecture remains.
Takeaway #7: Why We Choose “Familiar Pain” Over “Unfamiliar Freedom”
One of the most baffling aspects of self-destruction is why we return to things that hurt us. The answer lies in the brain’s prioritisation of Prediction over Well-being.
The nervous system is wired for the familiar. Stored patterns are “metabolically cheap” to run. The brain rewards pattern matching because the “Known” is, by definition, survivable—you have proof because you are still here.
The Comfort of the Wound: If you grew up in chaos, your nervous system calibrated to that frequency. As an adult, “Stability” feels suspicious. You might generate drama just to get back to a “Frequency” your machine recognises.
The Novelty Threat: Unfamiliar comfort contains no guarantee of survival. When things start going well, the brain interprets the stillness as an intolerable load or a “threat” because it has no template for it.
“Familiar pain is survivable. The nervous system has proof. Unfamiliar comfort contains no such guarantee.”
Recovery feels “wrong” not because it is bad, but because it is new. It is a calibration problem, not a motivation problem.
Conclusion: Picking Up the Wrench
If you have spent years trying to “think” your way out of your patterns, it is time for a different approach. You are not a patient in need of a cure, and you are not a sinner in need of redemption. You are a Mechanic who has been handed a machine with corrupted legacy code, running under a load it was never designed to carry alone.
The work of change doesn’t happen in the “Why.” It happens in the State. When an episode occurs, the Mechanic does not hold a Tribunal to deliver a verdict of shame; they conduct a Military Debrief. We don’t ask “Why am I so weak?” We ask, “What was the load? What was the Tone reading? Where did the trigger connect to the Installation? At what point did The Gate close?”
The Mechanic’s work involves:
Servicing the Hardware: Raising “Tone” through sleep, nutrition, and load management so The Gate stays open.
Reading the Data: Treating every relapse as diagnostic data about the current load.
Updating the Code: Using the repetition of new, managed experiences to recalibrate your nervous system to a new frequency.
At the back of Under Load by Ian Callaghan, you will find a 30-Day Field Manual: Reset the Machine. This is the technical manual for the work ahead. It doesn’t ask you to surrender; it asks you to look at the gauges, check the wiring, and start making the practical adjustments that allow the machine to run. You have spent long enough as a passenger in a vehicle steering itself toward a cliff. It is time to move into the driver’s seat.
Final Thought: If you stopped trying to think your way out of a state problem and started servicing the machine instead, what is the first load you would choose to set down?
The Emotional Mastery book is a practical manual for understanding and regulating the human nervous system using the Emotional Operating System framework.
Instead of analysing emotions or retelling your past, the Emotional Mastery book teaches you how to read emotional states as system feedback, identify overload, and restore stability under pressure.
No labels. No therapy-speak. No endless healing loops. Just a clear, operational approach to emotional regulation that actually holds when life applies load.
Used to monitor number of Google Analytics server requests when using Google Tag Manager
1 minute
_gid
ID used to identify users for 24 hours after last activity
24 hours
_ga_
ID used to identify users
2 years
_gali
Used by Google Analytics to determine which links on a page are being clicked
30 seconds
_ga
ID used to identify users
2 years
__utmx
Used to determine whether a user is included in an A / B or Multivariate test.
18 months
__utmv
Contains custom information set by the web developer via the _setCustomVar method in Google Analytics. This cookie is updated every time new data is sent to the Google Analytics server.
2 years after last activity
__utmz
Contains information about the traffic source or campaign that directed user to the website. The cookie is set when the GA.js javascript is loaded and updated when data is sent to the Google Anaytics server
6 months after last activity
__utmc
Used only with old Urchin versions of Google Analytics and not with GA.js. Was used to distinguish between new sessions and visits at the end of a session.
End of session (browser)
__utmb
Used to distinguish new sessions and visits. This cookie is set when the GA.js javascript library is loaded and there is no existing __utmb cookie. The cookie is updated every time data is sent to the Google Analytics server.
30 minutes after last activity
__utmt
Used to monitor number of Google Analytics server requests
10 minutes
__utma
ID used to identify users and sessions
2 years after last activity
_gac_
Contains information related to marketing campaigns of the user. These are shared with Google AdWords / Google Ads when the Google Ads and Google Analytics accounts are linked together.