The Invisible Pipeline: Why Your Health is a Managed Asset and How to Reclaim Your Metabolic Sovereignty
Introduction: The Exhaustion Paradox
Do you find yourself waking up already counting the hours until you can return to bed?
If you want the blunt framework for what’s happening, it’s the Food to Pharma Pipeline; the upstream food system creates the damage, and the downstream pharma system manages the fallout. You are not alone. Across the United Kingdom, from the frantic corridors of the City to the quietest suburban high streets, a peculiar and pervasive exhaustion has taken root. It is a heavy, systemic fatigue that seems immune to the traditional advice of “just getting more sleep” or “drinking more water”. You might be the individual who diligently tracks their ten thousand steps, tries to choose the “healthy” salad bowl from a high-street chain, and perhaps even spends a significant portion of their income on gym memberships or high-end supplements. Yet, despite these efforts, the 3:00 PM slump remains an inevitable daily visitor, your brain feels clouded by a persistent, low-level fog, and your energy levels resemble a volatile stock market chart rather than a steady, reliable resource.
This is the Exhaustion Paradox. We live in an era of unprecedented medical advancement and nutritional abundance, yet we have never felt more depleted. The frustration is compounded by a nagging sense of personal failure. When the weight does not move, or when the hunger signals become so uncontrollable that you find yourself standing in front of the fridge at 11:00 PM, you are told, and you tell yourself, that it is a matter of willpower. We treat our health as a moral ledger, where every “slip-up” is a sign of weak character or lack of discipline.
Now the bit that matters for context and trust.
I’m Ian Callaghan, British Army veteran and professional chef, not the Liverpool football legend. I’ve spent four decades around food and how humans actually eat, not how a spreadsheet says they should. I’ve watched the standard advice fail normal people for years, and then I watched it fail me. When I finally changed the inputs and rebuilt the basics, real food, protein, sleep, movement, and nervous system regulation, the results were not mysterious.
However, the reality is far more clinical and, in many ways, more liberating once understood. Your struggle is not a moral failure. It is a predictable biological response to a meticulously engineered environment. We are currently operating within what can be described as the metabolic environment, a landscape where our ancient biological wiring is being systematically outmatched by modern industrial design.
The central thesis of our current health crisis is this. Our widespread ill-health and lack of vitality are not accidental. They are the logical, foreseeable outcomes of a dual-industry incentive structure that prioritises shareholder returns over human physiology. You are not failing the system. The system is functioning exactly as it was designed to, with your health as the managed asset in a very long, very profitable pipeline. To reclaim your sovereignty, you must first understand the infrastructure of the pipeline you are currently standing in.
The Food to Pharma Pipeline: Upstream food, downstream pharma
This section is the Food-to-Pharma Pipeline in plain English: how upstream inputs set the conditions and how the downstream system monetises the consequences. To understand why you feel the way you do, you must first visualise the Food-to-Pharma Pipeline. This is the invisible infrastructure that connects what we eat to how we are medically treated. This relationship is not a loose association. It is a perfectly aligned economic journey categorised into two distinct phases: the upstream and the downstream.
Upstream refers to the food environment. This is the point of entry for the vast majority of the inputs that dictate our metabolic health. It is dominated by a global food supply that has been industrialised to an extent previously unimaginable in human history.
Downstream refers to the medical economy, specifically the segment of the pharmaceutical industry dedicated to managing the chronic fallout from upstream inputs.
The Incentive Structure: Profit over Conspiracy
It is essential to clarify that this is not a “conspiracy theory” in the sense of masked figures meeting in darkened rooms to plot the decline of public health. Real-world systems are rarely that theatrical. Instead, this is a matter of an incentive structure.
In a capitalist framework, corporations have a fiduciary duty to maximise value for their shareholders. This is not just a business preference. In many jurisdictions, it is a legal requirement.
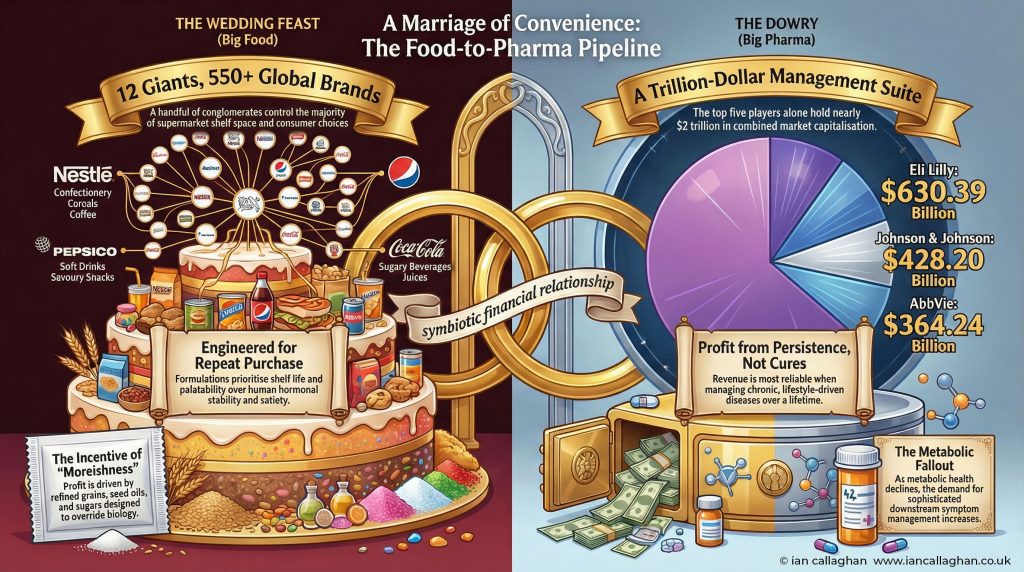
The food industry maximises value through shelf life, scalability, and moreishness, ensuring that products can be sold globally at low cost and high volume. The pharmaceutical industry maximises value through the long-term management of chronic conditions.
If you can create a food product that is cheap to produce and induces repeat purchase through chemical palatability, you have a successful business model. If you can then provide a medication that manages the biological disruption caused by that food, requiring daily use for years or even decades, you have another successful business model.
These two industries do not need to coordinate their efforts. They simply need to respond to the financial gravity of their respective markets. The pipeline is the natural result of these two profit models sitting side-by-side. Your metabolic dysfunction is the throughput that keeps the pipeline profitable.
Big Food and ultra-processed foods: the illusion of choice
This is the upstream half of the Food to Pharma Pipeline, where ultra-processed foods, seed oils and engineered palatability do the heavy lifting. When you walk through a modern supermarket, the illusion of choice is overwhelming. Rows upon rows of different brands, vibrant colours, and sophisticated health claims greet you at every turn. However, this diversity is largely superficial.
The vast majority of items found in the average supermarket trolley are controlled by a tiny cluster of global giants. Ten conglomerates effectively act as the gatekeepers of the modern diet. Nestlé, PepsiCo, Unilever, Coca-Cola, Mars, Danone, General Mills, Kellogg’s, Associated British Foods, and Mondelēz.
These companies do not design products primarily around human satiety or hormonal stability. To do so would be to ignore their primary mandate of growth. Instead, their engineering focuses on four key pillars that are fundamentally at odds with human biology.
Cost efficiency
Using the cheapest possible raw materials. This almost always means a base of refined seed oils (like rapeseed or sunflower oil), refined grains, and various forms of industrialised sugar.
Shelf life
Ensuring products can sit in a warehouse, on a lorry, or on a supermarket shelf for months, or even years, without degrading. This requires the removal of volatile nutrients and the addition of stabilisers and preservatives.
Scalability
Creating formulations that can be manufactured at a massive scale and taste identical in London, New York, or Tokyo. This requires a level of processing that strips food of its natural complexity.
Palatability
Using sophisticated flavour systems and the bliss point (the perfect ratio of salt, sugar, and fat) to override the body’s natural stop signals.
The result is a food environment dominated by formulated foods, products that are not grown in the traditional sense, but assembled. These are sauces, spreads, cereal bars, and ready meals that are engineered to be moreish and keep you coming back for another hit.
By using refined sugars and fats in ratios that do not exist in nature, these companies have created a biological hijack. When you consume these products, you are not just eating. You are engaging with a product designed by chemists to ensure you do not feel full.
This is why willpower feels so futile. You are attempting to use the prefrontal cortex, the logical, modern part of your brain, to fight against ancient survival circuits in the hypothalamus that are being overstimulated by multi-billion-pound engineering. The gatekeepers have figured out how to bypass your satiety and go straight for your dopamine.
Big Pharma and chronic disease management: the downstream business
This is the downstream half of the Food to Pharma Pipeline, where chronic disease management becomes the business model. Once the food environment has done its work, creating the predictable pressure on the human system, the downstream phase of the pipeline begins. This is where the pharmaceutical industry steps in to manage the biological malfunction.
The Big 5 giants, Pfizer, Johnson & Johnson, Roche, Novartis, and Merck, alongside others like Eli Lilly and Novo Nordisk, dominate a medical economy that has become increasingly focused on chronic disease management.
The financial gravity of this system is enormous. Chronic metabolic illnesses, type 2 diabetes, hypertension, and non-alcoholic fatty liver disease, are incredibly lucrative because they require long-term, daily intervention. From a shareholder’s perspective, a patient who manages their symptoms with a daily pill or a weekly injection for thirty years is a far more reliable asset than a patient who fixes their inputs and no longer requires the product.
This brings us to the modern nuance of GLP-1 medications (such as Ozempic or Wegovy). These drugs are a marvel of biotechnology and are appropriate and necessary in certain clinical cases to reduce appetite and improve glycaemic control.
However, we must be honest about their role in the pipeline. They are not a population-level fix for a fundamentally mismatched food environment. If the upstream drivers, the refined oils, the sugar-laden snacks, and the sedentary lifestyle, remain untouched, the demand for these drugs becomes permanent.
We are entering an era of sophisticated management, where we use expensive, high-margin medications to quiet the food noise created by high-margin, ultra-processed foods. It is a closed loop of consumption in which the individual remains a customer at both ends of the pipeline.
The medical economy has become exceptionally good at patching the holes created by the food industry. Still, it is structurally unaligned with closing the pipeline at the source because doing so would eliminate enormous and reliable revenue at scale.
Why your biology is outmatched by design: seed oils, sugar, refined grains
This is the mechanism inside the Food to Pharma Pipeline, the inputs create predictable metabolic dysfunction long before anyone calls it a diagnosis. The shift from real food to formulated inputs is the primary driver of our metabolic crisis. For the vast majority of human history, our biology interacted with whole, complex structures, meat, fish, tubers, seasonal fruits, and vegetables. These foods came with built-in data for the body, fibre to slow digestion, micronutrients to facilitate chemical reactions, and protein to signal satiety.
The modern era has seen this replaced by a trinity of metabolic disruptors.
Refined seed oils
Industrialised fats that are high in omega-6 and prone to oxidation, creating a state of systemic inflammation.
Refined grains
Flour that has been stripped of its fibre and germ, turning it into a rapid-fire glucose delivery system.
Added sugars
Specifically high-fructose loads that bypass the standard satiety signals and go straight to the liver for processing.
When these ingredients become the default fuel source, they exert a predictable pressure on human physiology. The most common manifestation of this pressure is insulin resistance. When the body is flooded with refined glucose and fructose multiple times a day, the pancreas must pump out massive amounts of insulin to clear the blood. Over time, the cells become deaf to the signal.
This leads to a state in which insulin levels remain chronically elevated, effectively locking fat cells and making it biologically difficult to access stored energy (body fat) as fuel. This is why people can be overweight yet feel starved of energy.
Furthermore, we are seeing a crisis of fatty liver. The source material notes that 40% of the population is developing fatty liver, a condition once reserved for heavy drinkers but now rampant in children and teetotal adults. This is a direct result of the liver being overwhelmed by refined sugars.
In this landscape, shelf space is the primary enemy of metabolic health. The more space a supermarket dedicates to items with a long shelf life, the more metabolic friction is introduced to the population. The industrial speed and chemical complexity of these modern inputs simply outmatch our biology.
Acute care vs chronic management: where medicine shines, and where it stalls
This is where the Food to Pharma Pipeline hides in plain sight, acute medicine is brilliant, but chronic prevention is structurally misaligned. One of the most important nuances to understand in the metabolic health conversation is the distinction between two very different types of medicine. It is vital to maintain a clear line here to avoid falling into unhelpful cynicism.
Modern medicine, especially acute care, is one of the greatest achievements in human history. If you are facing an emergency, sepsis, a car accident, a broken limb, a stroke, or a complex surgery, the current medical system is unparalleled. We should all want that system firing on all cylinders in a crisis. The surgeons, nurses, and emergency physicians operating in this space are literal lifesavers.
However, a problem arises when we attempt to use the acute care model, which is designed for find a bug, give a drug or fix a break, to treat the slow, grinding rise of lifestyle-driven chronic disease.
As the source states, the system is extremely good at managing illness and far less structurally aligned with preventing it at scale.
The crisis we face today is not a lack of emergency rooms. It is the fact that our primary mode of healthcare has become the management of diseases that are fundamentally caused by our environment.
We are using 21st-century medicine to treat 19th-century lifestyle problems, too much energy, too little movement. Because management is more profitable and easier to standardise than the unsexy work of lifestyle intervention, the pipeline remains the dominant structure.
The system is designed to keep you alive and consuming, but not necessarily to make you vital and independent.
The willpower myth: why food noise isn’t a character flaw
The Food to Pharma Pipeline relies on you blaming yourself, because self-blame keeps the upstream and downstream purchases flowing. One of the most damaging aspects of the current metabolic health crisis is the narrative of willpower. We have been led to believe that obesity and metabolic dysfunction are moral failings, that if people just tried harder or had more discipline, the problem would vanish. This is the eat less, move more mantra that has failed for four decades.
This narrative serves as a convenient shield for the industries involved. If the problem is your lack of character, then the food companies are not responsible for their moreish engineering, and the pharmaceutical companies are simply helping you deal with the consequences of your choices.
In reality, the modern food environment is engineered to override normal satiety signals. Our biological wiring is designed for a world of scarcity, where we are driven to seek out calorie-dense foods to survive the winter. When you place that ancient wiring in a world of infinite, ultra-processed abundance, the result is a mismatch.
Your brain is being chemically persuaded to overconsume through a flood of dopamine and a suppression of leptin (the satiety hormone). For most people, this is not a willpower problem. It is a chemistry problem.
You cannot will your way out of a hormonal cascade triggered by industrialised food formulations. To fix the behaviour, you must first fix the biology by changing the inputs.
High-margin products vs the unsexy truth: what actually fixes metabolism
If you want out of the Food to Pharma Pipeline, this is the part that matters, the boring foundations beat the high-margin fixes. There is a stark economic contrast between high-margin consumables, the products that drive quarterly earnings for conglomerates, and the unsexy foundations of genuine health.
The things that actually move the needle for human vitality are, by their very nature, difficult to monetise. You cannot put a high-margin patent on a good night’s sleep, a home-cooked steak, or a walk in the park.
Because these foundational shifts do not create predictable revenue curves or lifetime dependency, they are often ignored or sidelined in the public health conversation. They are boring because they require effort and do not come in a shiny package with a marketing budget behind them.
The boring foundations of metabolic sovereignty
Cooking basic ingredients. Taking control of the inputs by moving away from pre-packaged formulations. When you cook a piece of meat and a vegetable in butter or olive oil, you eliminate the gut chaos of industrial stabilisers.
Muscle maintenance. Perhaps the most underrated tool. Muscle is not just for aesthetics. It is a vital metabolic organ. It acts as a glucose sink, soaking up excess blood sugar and improving insulin sensitivity even at rest.
Prioritising protein. Ensuring the body has the structural building blocks it needs. Protein is the most satiating macronutrient. Prioritising it is the fastest way to silence food noise naturally.
Sleep quality. Viewing sleep as a non-negotiable recovery phase. Poor sleep immediately disrupts insulin sensitivity and spikes hunger hormones the following day.
Reducing alcohol. Being honest about how alcohol disrupts the nervous system, prevents fat oxidation, and increases systemic inflammation.
From a quarterly earnings perspective, these solutions are a disaster. They require less spending, less consumption, and more self-reliance. But from a biological perspective, they are the only things that work to dismantle the pipeline from the inside out.
Stepping off the pipeline: what changes when you fix inputs
Stepping off the Food to Pharma Pipeline is not about perfection, it’s about removing the inputs that keep you trapped in symptom management. Personal transformation is the ultimate proof of concept. The author of the source material provides a powerful example of what happens when one chooses to step off the pipeline.
After forty years of living within the standard modern pattern, experiencing the five-stone weight gain, the erratic energy, and the nonsensical hunger that plagues so many, the author shifted to an ancestral, lower-processing approach.
By focusing on real food, proper protein, and the boring foundations, the results were not just weight loss, but a complete physiological reboot. Hunger signals calmed down, and energy steadied. This was not due to magic or a secret supplement. It was the result of removing metabolic friction.
When you stop flooding the body with conflicting, industrial signals, the human system is remarkably responsive. The body wants to be healthy. It just needs the right data.
As the text emphatically states, this isn’t healthcare. It’s a pipeline. Step off it.
The goal is to move from being a managed asset in a corporate ecosystem to being a sovereign individual with a functioning metabolism. This shift occurs the moment you realise that you have more control over the inputs than the gatekeepers want you to believe.
Stepping off the pipeline does not mean perfection. It means choosing a different direction of travel.
The 2026 roadmap: metabolic flexibility and nervous system regulation
This is the exit strategy from the Food to Pharma Pipeline, fuel switching plus nervous system regulation, built on real food and real habits. Reclaiming your health in 2026 and beyond requires a tactical roadmap that prioritises biological independence over symptom management. This is about moving from a wired and tired state to one of regulated, reliable energy.
There are two key concepts to master.
Fuel switching (metabolic flexibility)
Most people in the modern world are sugar burners. Because their insulin is chronically high, they cannot access their body fat for fuel. They are like a petrol tanker that has run out of fuel but cannot access the 30,000 litres in the back.
Fuel switching is the process of training your body to switch between burning glucose and stored fat efficiently. This is achieved by stabilising insulin through real food and protein-forward eating, allowing the body to regain its natural metabolic flexibility.
Nervous system regulation
Metabolic health is not just about what you eat. It is about how your body perceives the world.
Chronic stress keeps the body in a state of high cortisol, which raises blood sugar and prevents repair. Regulation involves moving from a state of survival to a state of safety, where the body can prioritise metabolic maintenance.
This involves managing the gut chaos caused by additives and using movement and sleep to calm the nervous system.
This roadmap involves a military-grade focus on the basics. Silencing food noise by choosing high-satiety proteins and whole foods, and removing the industrial seed oils that hammer the system every day.
By consistently changing the input, you allow your physiology to follow its natural design. You stop white-knuckling your way through hunger and start working with your biology instead of against it.
Conclusion: A Final Thought for the Shareholder
The Food to Pharma Pipeline is profitable because it keeps people tired, hungry and reliant, and it stays profitable until enough people change the inputs. The Food to Pharma landscape is a marvel of economic efficiency, but it is a catastrophe for human vitality.
We are currently living in a world where our health is outsourced to industries whose primary duty is not to our well-being, but to their shareholders.
Every time we choose a highly processed, convenient meal, we are feeding the upstream.
Every time we rely solely on a pill to manage the resulting metabolic friction without addressing the cause, we are feeding the downstream.
The most productive question you can ask yourself today is not which diet should I try, or is there a new drug for this.
The real question is, are you ready to stop managing symptoms and start fixing inputs?
Are you willing to stop being an asset in someone else’s pipeline and start being the sovereign of your own biology?
The tools for this reclamation are not found in a laboratory or a factory. They are found in the unsexy decisions you make in your kitchen, your bedroom, and your daily movement.
The system is perfectly designed to keep you exactly where you are, tired, hungry, and reliant.
The only way out is to step off the pipeline and take back the wheel.
Whether you are ready to engage in a 30 Day Reset to calm the gut chaos or you are seeking a long-term roadmap to metabolic sovereignty, the path remains the same. Change the inputs, and the physiology will follow.
The question is no longer whether the system will change for you, but whether you will finally choose to change for yourself.
Introduction: The Relatable Illusion of the Quick Fix | GLP-1 weight loss side effects
GLP-1 weight loss side effects. In the history of metabolic medicine, few developments have ignited a global frenzy comparable to the rise of glucagon-like peptide-1 receptor agonists, or GLP-1RAs. Known popularly by brand names such as Ozempic, Wegovy, and Mounjaro, these agents have moved from specialist type 2 diabetes treatments to widely promoted weight-loss solutions. The public narrative is seductively simple: a once-weekly injection that quiets intrusive food noise, slows the stomach and reduces body fat with striking efficiency.
However, as so-called Ozempic fever reaches a tipping point, a more complex clinical reality is emerging from longitudinal studies and pharmacovigilance data. While the drop on the weighing scale is real, the physiological cost of rapid weight reduction remains under-discussed in mainstream conversations. The central question is no longer whether these drugs work. They clearly do. The real question is the quality of the weight lost and what happens to the metabolic system over time.
Key Definition: What is a GLP-1 drug?
GLP-1 receptor agonists are medications that mimic the natural gut hormone glucagon-like peptide-1. They reduce appetite, slow gastric emptying, and improve blood glucose control. Drugs in this class include semaglutide, sold as Wegovy and Ozempic, and tirzepatide, sold as Mounjaro, which also targets the GIP receptor.
Takeaway 1: The “1 in 10” Experiment – A Public Health Tipping Point
The adoption of GLP-1 receptor agonists has reached a scale that materially alters the public health landscape.
In the United States, survey and claims data from 2024 to 2025 show rapid growth. Around 12 per cent of adults reported current use by late 2025, with approximately 18 per cent reporting that they had used a GLP-1 drug at some point.
In Great Britain, usage remains lower but is rising quickly. Recent modelling suggests the broader GLP-1 economy now touches roughly one in ten adults when current use, recent use and stated intent are combined.
This represents a large real-world exposure population relative to the length of long-term safety data currently available.
US vs UK Usage Trends and Demographics
Metric
United States (2024 to 2025)
Great Britain (2025 estimates)
Current usage rate
Approximately 12 percent of adults
Approximately 2.9 percent for weight loss
Ever used
Approximately 18 percent of adults
Approximately 4.5 percent past-year use
Primary demographic
Age 50 to 64 highest uptake
Age 30 to 49 strong private uptake
Gender pattern
Higher use in women
Majority female private prescriptions
Access barrier
Affordability concerns common
Lower access in deprived areas
A further concern in the UK is the fragmentation of prescribing data. A significant proportion of weight-loss prescribing occurs through private online providers, and these prescriptions are not always fully integrated into GP records. This creates a potential pharmacovigilance blind spot for national safety monitoring.
Takeaway 2: The Gastrointestinal Reality – When “Nausea” Becomes Pathological
The most common adverse effects of GLP-1 receptor agonists are gastrointestinal. Mechanistically, this is expected because the drugs intentionally slow gastric emptying and alter gut motility.
Clinical trials often describe these effects as mild to moderate. In real-world use, a subset of patients experience significant functional impairment.
Of particular concern is drug-induced gastroparesis, where gastric emptying becomes severely delayed.
Research with liraglutide has demonstrated substantial prolongation of gastric emptying time in some individuals, with downstream risk of persistent nausea, vomiting of undigested food and reduced oral intake.
Common Gastrointestinal Side Effects
Nausea: approximately 20 to 50 per cent
Diarrhoea: approximately 10 to 34 per cent
Vomiting: approximately 10 to 20per centt
Constipation: approximately 5 to 1 per cent
Abdominal pain: approximately 5 to per cent
Dyspepsia or reflux: approximately 1 toper centcent
Regulators in both Europe and the UK have also added warnings regarding ileus and bowel obstruction, with frequency currently classified as unknown.
Takeaway 3: Serious Clinical Risks in the Safety Data
Beyond gastrointestinal effects, several clinically significant risks appear in regulatory labelling and post-marketing surveillance.
Clinical Red Flags
Acute pancreatitis. A recognised class risk. UK regulators advise immediate discontinuation if suspected.
NAION, non-arteritic anterior ischaemic optic neuropathy. A rare but potentially permanent form of vision loss is under investigation.
Acute kidney injury. Often secondary to dehydration from persistent vomiting or diarrhoea.
Biliary disease. Rapid weight loss increases the risk of gallstones and cholecystitis.
Thyroid C-cell tumours. Observed in rodent models. Human relevance remains uncertain, but these drugs remain contraindicated in patients with a relevant cancer history.
Pulmonary aspiration risk. Delayed gastric emptying increases anaesthetic risk if stomach contents are retained.
Regulatory emphasis varies slightly between regions, but these risks are present in official product information.
Takeaway 4: The Sarcopenic Risk – Losing Lean Mass
One of the most important clinical questions is body composition change, not scale weight alone.
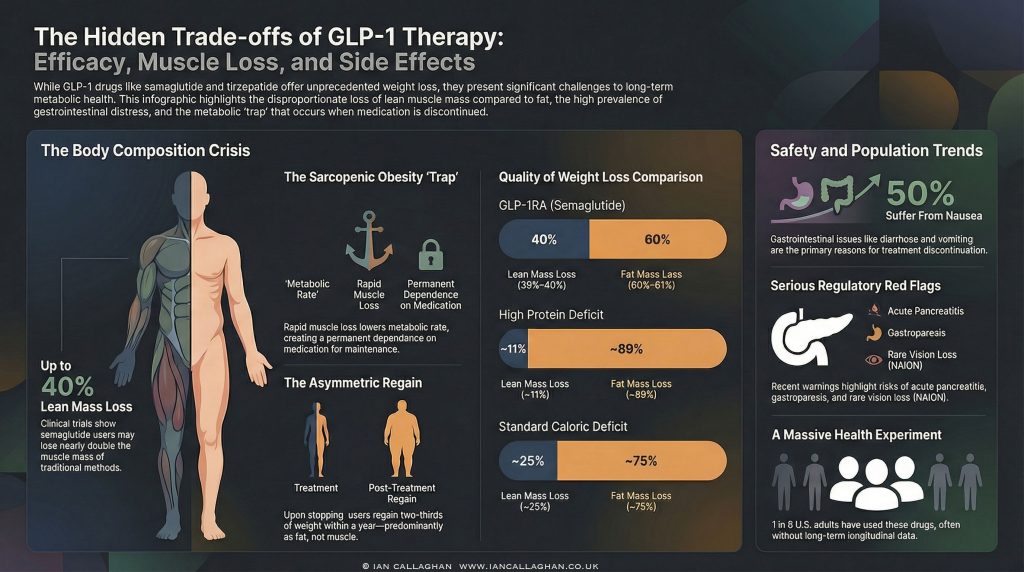
In traditional weight loss, approximately 25 per cent of the weight lost is lean mass. GLP-1 trials show variable, and sometimes higher, lean mass loss, particularly when protein intake and resistance training are not optimised.
In the STEP 1 semaglutide trial, participants lost on average 6.9 kg of lean mass at 68 weeks. This represented roughly 39 to 40 per cent of total weight lost in that cohort.
Weight Loss Method vs Lean Mass Loss
Method
Lean mass loss
Fat mass loss
Context
GLP-1 semaglutide
Approximately 39 to 40 percent
Approximately 60 percent
Rapid pharmacological deficit
Tirzepatide
Approximately 25 to 34 percent
Approximately 66 to 75 percent
Dual agonist effect
Bariatric surgery
Approximately 23 percent
Approximately 77 percent
Surgical intervention
Standard dieting
Approximately 25 percent
Approximately 75 percent
Behavioural deficit
High protein protocol
Approximately 11 percent
Approximately 89 percent
Muscle-preserving approach
Loss of skeletal muscle has metabolic consequences because muscle is a major driver of resting energy expenditure and glucose disposal. In particular, among older adults, excessive loss of lean mass is associated with increased risk of frailty.
Takeaway 5: The Post-Cessation Regain Problem
Data from the STEP 1 extension study showed that after stopping semaglutide, participants regained roughly two-thirds of their prior weight loss within one year.
Body composition of regained weight varies by individual and by behaviour after cessation. However, from a physiological standpoint, fat mass typically returns more readily than lean mass unless deliberate resistance training and adequate protein intake are maintained.
Key Biological Drivers of Regain
Ghrelin rebound, increasing hunger signals
Leptin suppression relative to body weight
Reduced resting energy expenditure following lean mass loss
Together, these factors create a strong biological drive toward weight regain if lifestyle structure is not in place.
Takeaway 6: The UK Access Gap
In the United Kingdom, NICE modelling suggests that millions may meet the eligibility criteria for newer agents, such as tirzepatide. However, the phased NHS rollout currently limits access to a much smaller cohort.
This has driven the rapid expansion of the private prescribing market.
Evidence suggests lower prescribing rates in more deprived regions despite higher obesity prevalence, highlighting a widening access gap.
Key Structural Pressures
NHS capacity constraints
Private prescribing costs
Fragmented data reporting
Higher entry BMI in more deprived populations
Takeaway 7: Muscle Preservation Is Not Optional
Emerging clinical consensus is clear. Weight loss without planning for muscle preservation is suboptimal.
Current Best Practice Guardrails
Protein intake around 1.6 g per kg body weight per day
Regular resistance training
Monitoring of functional strength, where possible
The pharmaceutical pipeline itself reflects this concern. Combination approaches designed to preserve or increase lean mass are already under investigation, including agents targeting activin pathways.
Conclusion: A Population-Level Trade-Off?
GLP-1 receptor agonists are powerful and clinically valuable tools in appropriate populations. They are not consequence-free.
Atthe population scale, the central issue is no longer simply weight reduction. It is metabolic quality, long-term dependence, preservation of lean tissue, and the behavioural vacuum that often sits beneath pharmacological appetite suppression.
The uncomfortable reality emerging from both trial data and real-world observations is this. These drugs address the intake side of the energy equation very efficiently, but they do not automatically address the structural drivers of metabolic dysfunction.
If protein intake is inadequate, lean mass falls. If resistance training is absent, muscle signalling drops. If lifestyle scaffolding is weak, pressure builds the moment the pharmacology is withdrawn.
For clinicians working in obesity medicine, this is not theoretical. It is already visible in follow-up cohorts.
The Dependence Question
One of the most under-discussed implications of widespread GLP-1 use is the shift towards chronic pharmacological weight maintenance.
Unlike short-term dieting tools, GLP-1 receptor agonists exert their effects primarily through modulation of appetite and changes in gastric motility. When the drug is withdrawn, the physiological environment that supported the lower body weight often reverses.
This raises three population-level questions that remain only partially answered:
What proportion of users will require long-term therapy to maintain weight loss?
What is the metabolic profile of patients five to ten years after initiation?
How will large-scale lean mass reduction in midlife populations affect frailty curves later on?
Long-term outcome data are still maturing.
The Behavioural Displacement Problem
Another emerging concern is behavioural displacement.
When appetite is pharmacologically suppressed, patients often eat less without necessarily improving dietary quality, protein distribution, micronutrient density or movement patterns. In some cohorts, this creates a situation in which weight declines while nutritional robustness does not improve in parallel.
From a purely clinical standpoint, weight loss without functional improvement is an incomplete win.
Markers that matter long term include:
Muscle strength
Physical function
Protein adequacy
Micronutrient status
Glycaemic stability post-treatment
These are not consistently tracked within the commercial weight-loss ecosystem.
The Private Prescribing Blind Spot
In the UK, especially, the rapid expansion of private GLP-1 prescribing has created a structural monitoring problem.
When treatment is initiated outside integrated NHS pathways, several risks increase:
Adverse events may not be fully linked to the medication in primary care records
Medication histories may be incomplete at hospital presentation
Long-term outcome tracking becomes fragmented
This is what pharmacovigilance specialists refer to when they discuss signal dilution in real-world data.
It does not mean the drugs are unsafe. It means the surveillance environment is imperfect and still evolving.
Who Clearly Benefits
It is equally important to state what the data does support.
In appropriately selected patients, GLP-1 receptor agonists can deliver:
Significant weight reduction
Improved glycaemic control
Cardiometabolic risk improvement in defined populations
For patients with type 2 diabetes, severe obesity with complications or high cardiometabolic risk, these agents can be clinically transformative when properly supervised.
The concern raised in this analysis is not about legitimate medical use. It is about scale, context, and implementation quality in the rapidly expanding weight-loss market.
The Real Strategic Question
The global rollout of GLP-1 therapies represents one of the largest metabolic interventions in modern medicine.
The short-term efficacy story is clear. The long-term systems story is still being written.
If lean mass preservation, resistance training, protein adequacy and structured exit planning become standard practice alongside prescribing, outcomes may remain strongly positive.
If they do not, we may see a growing cohort of patients who are lighter on the scale but metabolically more fragile than their headline weight loss suggests.
That is the trade-off now under quiet scrutiny inside obesity medicine.
The scale is moving.
The deeper question is what else is moving with it.
FAQ: GLP-1 Drugs, Weight Loss and Muscle Loss
Do GLP-1 drugs cause muscle loss?
They can. Clinical trials show that a proportion of the weight lost with GLP-1 receptor agonists is lean mass. The amount varies by individual and is strongly influenced by protein intake, resistance training, age and total calorie deficit. Without active muscle-preservation strategies, lean mass loss can be significant.
Is the weight regain after stopping GLP-1 mostly fat?
Evidence shows substantial weight regain after discontinuation in many patients. Physiologically, fat mass tends to return more readily than lean mass unless structured training and nutrition are maintained. Body composition outcomes after cessation vary widely depending on lifestyle behaviour.
Are GLP-1 drugs safe for weight loss?
For appropriately selected patients under medical supervision, GLP-1 receptor agonists can be effective and clinically appropriate. However, they carry known side effects and risks, including gastrointestinal symptoms, pancreatitis risk, gallbladder disease and rare but serious complications. They are not risk-free cosmetic tools.
Who should seriously consider GLP-1 therapy?
Current clinical guidance generally supports use in:
Type 2 diabetes with inadequate control
Obesity with significant comorbidities
High cardiometabolic risk patients under supervision
Use purely for cosmetic weight loss requires careful risk-benefit consideration.
The Sovereign Operator Bundle gives you the full system. Three complete books plus 24/7 access to AI Ian, trained on over 40 years of real-world experience in nutrition, behaviour change and metabolic health.
Inside, you get the full EOM framework, the same principles Ian uses with clients to rebuild regulation, food control and metabolic resilience from the ground up.
This is not surface-level weight loss fluff. It is the operating manual.
Seed oil toxicity isn’t some fringe internet theory. It’s a question more and more people are quietly starting to ask as metabolic syndrome, insulin resistance, and chronic inflammation continue to explode across the modern world.
Look at a magazine from the 1950s. You’ll find full-page ads featuring men in crisp white lab coats, stethoscopes draped around their necks, confidently telling the American public that Camels soothe your T-zone and that more doctors smoke Chesterfields than any other brand.
We look back now and laugh. We think, how could they be so fucking blind? How could the medical establishment endorse the inhalation of carcinogenic smoke as a health practice?
Wipe that smug smile off your face. We aren’t any smarter today. A different master is just poisoning us.
Instead of Philip Morris, it’s the edible oil industry. Instead of tar in the lungs, it’s refined factory oils infiltrating every cell membrane in your body. The American Heart Association stamping its “Heart-Healthy” seal of approval on a bottle of highly refined, hexane-extracted, bleached, and deodorised canola oil is the same kind of deception as the doctor endorsing a carton of cigarettes. In fact, it might be worse.
Tobacco drives oxidative stress and DNA damage primarily through the respiratory and cardiovascular systems. Seed oils are different. They are structural. They become part of you. And if the mechanism is what many researchers argue it is, they can contribute to systemic oxidative stress, mitochondrial dysfunction, and chronic inflammation across multiple tissues. Seed oil toxicity isn’t just the new tobacco. It’s one of the biggest uncontrolled nutrition experiments ever run on humans. And you’re the lab rat.
If you’ve read my books, you know I don’t deal in diluted, sanitised fairy tales. I deal in mechanics. I deal in the raw truth of ancestral biology. So let’s tear the lid off this and look at the biochemistry of why your ancestors didn’t even have a name for metabolic syndrome.
THE ANCESTRAL BLUEPRINT: BOB THE CHIMP DOESN’T NEED A STATIN
To understand the absurdity of the modern diet, we need to talk about Bob the Chimp.
Bob doesn’t track his macros. Bob doesn’t have a continuous glucose monitor strapped to his arm. Bob doesn’t take 40mg of atorvastatin to keep his lipid panel looking pretty for his annual physical. Bob eats his species-specific diet. He forages, he eats, and his biology functions as nature intended.
When our hominin ancestors split from the primate lineage, we underwent a major evolutionary shift in digestion and metabolism. We traded the massive fermentative cecum of the ape for a larger small intestine. We stopped spending our days grinding tough fibrous leaves and became hunters. We ate the fat, the organs, the marrow, and the brains. We fuelled brain expansion not on kale or soybean oil, but on dense, stable animal fats.
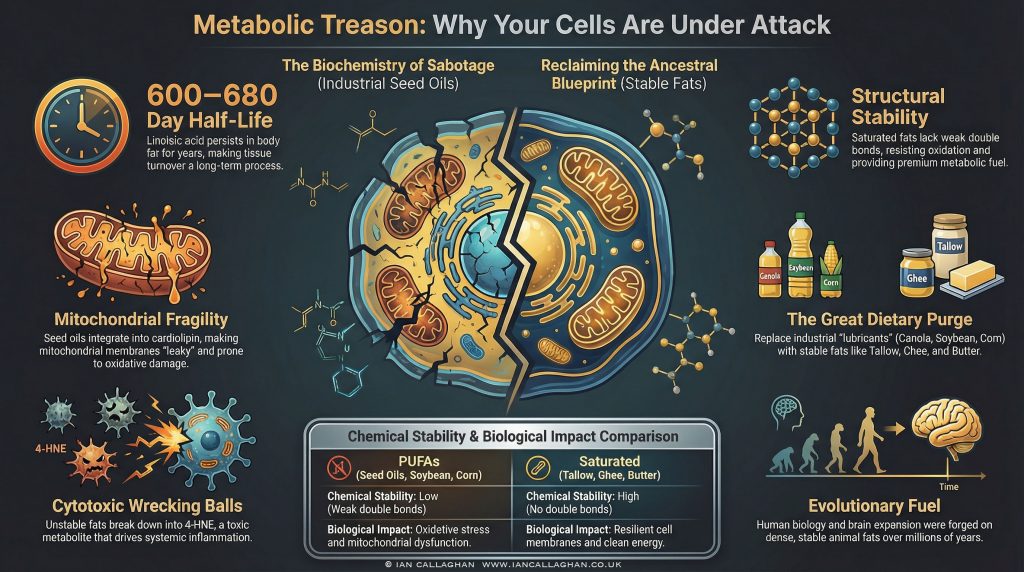
Our engine was forged over millions of years to run on stable lipids. Saturated fats have no double bonds in their carbon chains. They are structurally sound. They resist oxidation and are far less prone to forming nasty by-products when exposed to heat and oxygen. They are premium fuel for an ancient metabolic machine.
For most of human history, metabolic syndrome as a population-wide condition didn’t exist. Obesity was rare. Type 2 diabetes was uncommon. Heart disease was not the normal midlife “expected outcome”. Then came industrial processing, and with it, the great dietary swap.
THE BIOCHEMISTRY OF POISON: SEED OILS AND THE MITOCHONDRIAL ENGINE
Let’s get technical. Because if you don’t understand the sabotage, you stay vulnerable to it.
Seed oils (soybean, corn, canola, cottonseed, sunflower, safflower) are rich in linoleic acid (LA), an 18-carbon omega-6 polyunsaturated fatty acid (PUFA). Unlike saturated fats, linoleic acid contains multiple double bonds. In organic chemistry, double bonds are weak points. They’re more reactive and more prone to oxidation.
When you consume linoleic acid, your body incorporates it into your cellular architecture. It becomes part of your cell membranes. More importantly, it can become part of the inner mitochondrial membrane, including a crucial phospholipid called cardiolipin.
Cardiolipin helps organise and stabilise the electron transport chain. It supports the membrane environment, allowing efficient ATP production. When cardiolipin is built mostly from stable fats, the membrane stays resilient, and the system runs cleaner.
But when the diet is flooded with fragile PUFAs, cardiolipin can become more vulnerable to lipid peroxidation. Those double bonds are more easily damaged under oxidative stress. The membrane becomes leakier. The machinery becomes less efficient. The electron transport chain can become more uncoupled.
When that happens, mitochondria can generate more reactive oxygen species (ROS). Peroxidised linoleic acid can break down into reactive aldehydes, including 4-hydroxynonenal (4-HNE), and other oxidised linoleic acid metabolites (OXLAMs).
4-HNE is a microscopic wrecking ball. It’s cytotoxic. It can bind to proteins, impair mitochondrial function, and contribute to a cascade of inflammation and metabolic stress. Your cells can end up in a brutal contradiction: surrounded by energy, but struggling to generate it cleanly.
This is one plausible pathway into insulin resistance. Fat cells can become overloaded with oxidative stress and dysfunctional energy handling, and they begin to resist further storage as a protective response. Insulin resistance isn’t automatically a “genetic flaw”. In many cases, it’s a defensive adaptation to a toxic environment.
ENTER GLUCIPHER: THE ARCHITECT OF METABOLIC SABOTAGE
You can’t discuss seed oils without talking about the wider con. In my work, I call the architect Glucipher.
Glucipher is metabolic sabotage personified. The whisper in the ear of institutions. The invisible hand behind “heart healthy” marketing. The trickster who convinced people to eat factory oils instead of the fats that built our brains.
Glucipher doesn’t just want you fat. Fat is a side effect. Glucipher wants your cells broken, your appetite dysregulated, your energy unstable, and your hunger permanently switched on.
How did this con get traction? Mid-20th-century nutrition politics. Demonisation of saturated fat, a public-health narrative built on contested data and aggressive messaging. The Seven Countries Study is still debated for its limitations and the conclusions people drew from it. The result was a cultural swap: butter and tallow became “bad”, and seed oils became “good”.
And then came the unholy alliance: seed oils plus refined carbohydrates. If mitochondrial function is compromised, appetite signals can go feral. If you’re stuck in cellular stress, what do you crave? Quick energy. Sugar. Starch. Constant hits.
You eat more, you store more, you crash more. You get hungrier, not satisfied. Glucipher traps you in a loop of eating, storing, and starving.
THE HALF-LIFE OF A BIOLOGICAL BOMB
Here’s a major difference between tobacco and seed oils.
Smoke is exposure. Seed oils are structured.
Linoleic acid can persist in adipose tissue for a long time, with estimates often cited in the range of 600 to 680 days for turnover. That means if you stop right now, it can still take years for tissue composition to shift meaningfully.
Every time you burn fat, you can release stored fatty acids back into circulation. If those fats are more oxidation-prone, they can contribute to oxidative stress and inflammatory signalling as they move through the system.
Our ancestors likely obtained a small percentage of their energy from linoleic acid, enough for basic signalling. Modern diets can push that far higher, largely through ultra-processed foods, restaurant oils, and “healthy” packaged rubbish.
And then the system acts confused. “Why are people inflamed?” “Why is insulin resistance exploding?” “Why is metabolic dysfunction everywhere?” So the machine prescribes statins, GLP-1s, blood pressure meds, and more pills, while still telling people to cook with canola.
It’s metabolic treason.
RECLAIMING THE ENGINE
This part is the good news because it’s in your hands.
You cannot out-medicate a diet built on refined industrial oils. You cannot outrun mitochondrial dysfunction with a few steps and a green smoothie. You can’t biohack a structural problem while still building your body out of unstable inputs.
Metabolic syndrome isn’t “just ageing”. It’s not inevitable. It’s often the predictable outcome of putting volatile fuel into an ancient engine.
To break free, you return to ancestral inputs and modern common sense. You cut industrial seed oils hard. No soybean. No canola. No corn. No sunflower. No safflower. No grapeseed.
You cook with what the human animal actually evolved around. Tallow. Ghee. Butter. Suet. You give mitochondria stable building blocks. You lower oxidative load. You let the system rebuild.
The medical establishment lied about tobacco for decades. They’ve been wrong before. Don’t outsource your biology to institutions that get funded by the same industries selling you the problem.
Stop eating industrial lubricants. Reclaim your metabolic birthright.
Used to monitor number of Google Analytics server requests when using Google Tag Manager
1 minute
_gid
ID used to identify users for 24 hours after last activity
24 hours
_ga_
ID used to identify users
2 years
_gali
Used by Google Analytics to determine which links on a page are being clicked
30 seconds
_ga
ID used to identify users
2 years
__utmx
Used to determine whether a user is included in an A / B or Multivariate test.
18 months
__utmv
Contains custom information set by the web developer via the _setCustomVar method in Google Analytics. This cookie is updated every time new data is sent to the Google Analytics server.
2 years after last activity
__utmz
Contains information about the traffic source or campaign that directed user to the website. The cookie is set when the GA.js javascript is loaded and updated when data is sent to the Google Anaytics server
6 months after last activity
__utmc
Used only with old Urchin versions of Google Analytics and not with GA.js. Was used to distinguish between new sessions and visits at the end of a session.
End of session (browser)
__utmb
Used to distinguish new sessions and visits. This cookie is set when the GA.js javascript library is loaded and there is no existing __utmb cookie. The cookie is updated every time data is sent to the Google Analytics server.
30 minutes after last activity
__utmt
Used to monitor number of Google Analytics server requests
10 minutes
__utma
ID used to identify users and sessions
2 years after last activity
_gac_
Contains information related to marketing campaigns of the user. These are shared with Google AdWords / Google Ads when the Google Ads and Google Analytics accounts are linked together.