Why Your Sleep Tracker is a Liar: Reclaiming the Human System in a High-Tech World
1. Introduction: The Exhaustion Paradox
Imagine the scene: it is 11:45 pm, and you are lying in a bed that cost more than your first car, surrounded by a forest of tangled white USB cables—the digital umbilical cords of the modern age. On your wrist sits a high-precision titanium ring, and on your nightstand, a smartphone hums with the vibrating notifications of a world that never sleeps. The room is cool, the sheets are Egyptian cotton, and the air is purified to a laboratory standard. Yet, you are lying there, staring at the ceiling, feeling a strange, vibrating hum in your very bones. You are “tired but wired.”
This is the quintessential modern haunting. Your body is heavy, your eyes are stinging, and your brain feels like it has been scrubbed with steel wool, yet your nervous system refuses to disarm. You check your sleep tracker, hoping for a “Readiness Score” that might validate your suffering, but the data feels like a mockery. You have spent thousands of pounds on gadgets designed to “optimise” your rest, yet you wake up every morning feeling like a ghost of your former self.
Despite our unprecedented connectivity and our obsession with biohacking, we have never been more depleted. We download “bloody apps” to tell us why we are tired, then stay awake using those very apps to scroll through the curated lives of strangers, bathing our retinas in the blue light of a thousand miniature suns. This is the exhaustion paradox. We treat our bodies like high-performance machines that require constant surveillance, yet we ignore the fundamental, non-negotiable biological requirements of the system.
We have reached a point where the average professional is living like a mobile phone hovering at 1 percent battery. You are flickering, the screen is dimming, and the apps are crashing. Eventually, the system shuts down unexpectedly. You call this “recovery” because the screen went black and you stayed in bed for eight hours, but it is not recovery. It is a system failure. Real sleep isn’t a metric to be tracked, a “hack” to be mastered, or a point of negotiation. It is a biological system that must be respected. To reclaim your energy, you must stop looking at the scoreboard and start returning to your factory settings.
There is a profound, often ignored difference between being asleep and being unconscious. In our metric-obsessed culture, we have conflated the two. We boast about “getting our eight hours” as if sleep were a commodity you could buy in bulk at the supermarket. But we fail to examine the internal architecture of those hours. For many, sleep is not a graceful transition into the restorative rhythms of life; it is a violent, chemical collapse.
When you spend your day fueled by back-to-back stimulants and your evening suppressed by blue light, work-induced cortisol, and perhaps a “relaxing” glass of Malbec, you do not “fall” asleep. You pass out. You have pushed the human system to its absolute redline until it simply cannot maintain consciousness any longer. This is the “Phone on 1 Percent” state. When a phone dies because the battery is empty, it hasn’t “decided” to rest; it has suffered a total power loss.
“You pass out. You collapse. You go unconscious like a phone on 1 percent battery and call it recovery. That is not sleep. That is system failure.”
This system failure is the great delusion of modern health. We assume that as long as we were “out” for a certain duration, the body has performed its necessary maintenance—clearing metabolic waste, consolidating memories, and repairing tissue. But proper sleep is an active, complex, and highly choreographed biological process. It requires specific chemical and thermal conditions to occur. When we bypass these conditions through sheer exhaustion or chemical sedation, we wake up feeling “emotionally mugged,” despite the clock saying we spent nearly half a day in bed. We are confusing the absence of consciousness with the presence of recovery. True recovery is an investment in the architecture of the brain; sedation is merely a temporary ceasefire.
3. The Tracker Trap: Turning Your Body into a Disappointing Video Game
We have entered the era of “Scores for Scores.” We track steps, calories, heart rate variability, and blood glucose. We have sleep scores, readiness scores, and recovery scores. We have turned the miracle of 200,000 years of human evolution into a disappointing video game where you are constantly losing to an invisible opponent.
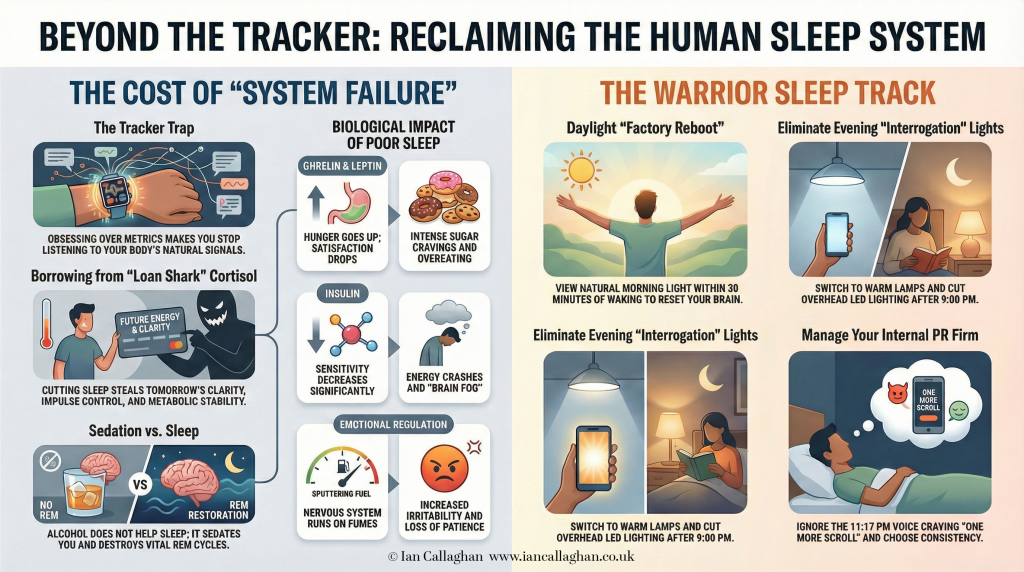
The psychological impact of this constant “scoring” is devastating to our innate biological intuition. By obsessing over metrics, we have effectively silenced the very signals our bodies use to communicate with us. We no longer ask ourselves, “How do I feel today?” Instead, we look at a ring or a watch to tell us if we are allowed to feel tired or energised. There is something deeply absurd about a grown adult looking at a piece of plastic to determine if they had a good night, while they are simultaneously “knackered and shouting at the kettle.”
This is the ultimate irony of the tracker trap: we use technology to negotiate with reality. We know that scrolling through social media at midnight under harsh LED lighting while answering “urgent” work emails is not restful behaviour. We know the wine we drank to “unwind” is a neurotoxin that shatters our sleep architecture. But we look for a “17 percent REM” score or a “Good” readiness rating to justify our choices, hoping the gadget will give us permission to ignore what our bodies are screaming at us.
Your tracker doesn’t know you. It knows your movement and your heart rate, but it doesn’t know the texture of your fatigue. When you obsess over the data, you become like a “distressed hamster” on a wheel, chasing a number that has no bearing on the underlying biological reality. The tracker becomes a way to outsource your intuition. You stop listening to the signals—the cravings, the brain fog, the irritability—and start chasing a performance. But health is not a performance; it is a state of being.
4. The Cortisol Loan Shark: The Brutal Interest of Sleep Debt
To understand why we feel so perpetually depleted, we must look at the brain for what it truly is: an electrical organ sitting in a dark, silent skull, running chemical software that was written in the Pleistocene. This ancient software does not care about your KPIs, your “4 am spreadsheet culture,” or your desire to be a “high-performer” on LinkedIn. It cares about survival, homeostasis, and the conservation of energy.
When you cut sleep to squeeze more productivity out of your day, you are not “gaining” an hour. You are entering into a predatory financial arrangement with your own biology. You are borrowing energy from tomorrow to pay for today’s inefficiency. The lender in this scenario is a hormone called cortisol—the “loan shark” of the human system.
Cortisol is the stress hormone designed to get you away from a predator or through a period of famine. It provides that artificial hit of “wired” energy that allows you to push through the fatigue, but the interest rate is brutal. By borrowing from the loan shark, you are forfeiting tomorrow’s clarity, your ability to control your impulses, and your metabolic stability.
This is why the “tired but wired” feeling is so pervasive in the city. You are living on high-interest biological debt. Your nervous system is running on fumes, propped up by a stress response that was never meant to be a permanent state of existence. You cannot out-hustle the basic requirements of a 200,000-year-old brain. Eventually, the loan shark comes to collect, and the payment is usually extracted in the form of a burnout, a breakdown, or a metabolic collapse.
5. The Hormonal Domino Effect: When Hunger and Emotion Go Feral
When sleep is compromised, the biological fallout is immediate, systemic, and unforgiving. It is a domino effect that touches every aspect of your humanity, from the food you choose to eat to the way you interact with your spouse. This isn’t a lack of “discipline” or a failing of “willpower”; it is a chemical hijacking.
The Hunger Imbalance (Ghrelin and Leptin) The moment you enter a sleep deficit, your hunger hormones go feral. Ghrelin, the hormone that signals hunger, spikes like a fever. Leptin, the hormone that signals fullness and satisfaction, plummets. This is why, after a poor night’s sleep, you find yourself in a “9 pm biscuit negotiation” with yourself. You are biologically programmed to seek out high-energy, sugary, hyper-palatable foods because your brain thinks it is in a survival crisis and demands immediate fuel. It is not a character flaw; it is “chemistry kicking your arse.”
The Metabolic Crash (Insulin Sensitivity) Poor sleep causes a rapid, measurable drop in insulin sensitivity. The biological reality is that the same meal you handled perfectly well a week ago—when you were rested—now hits your system like a metabolic brick. Your body cannot process the glucose effectively, leading to more blood sugar crashes, more intense cravings, and the pervasive sense of “why am I like this?” Your body’s ability to manage fuel effectively is tied directly to the quality of your rest. You cannot “green-smoothie” your way around a lack of sleep.
The Emotional Regulation Failure Finally, your emotional regulation tanks. The prefrontal cortex, the part of the brain responsible for impulse control, rational thought, and “being an adult,” loses its grip on the amygdala—the emotional centre of the brain. This is why small inconveniences—a slow lift, a misplaced set of keys, or a minor critique from a colleague—begin to feel like personal attacks. You are not actually angry at the world; you are simply under-recovered. Your nervous system is too frayed to provide the patience and focus required for modern life.
6. The Midnight Light Show: Why Your Brain Thinks It’s Noon in Ibiza
One of the greatest enemies of the human sleep system is the modern lighting environment. Our ancestors evolved under the rhythmic rising and setting of the sun, followed by the warm, dim, flickering glow of firelight. Our brains use light as the primary signal to determine what time it is and which hormones to produce.
Today, we subject ourselves to a “Midnight Light Show.” We inhabit homes filled with white LED kitchen lights that are “bright enough to interrogate prisoners.” We stare into laptops and phones that emit a specific spectrum of blue light that signals “High Noon” to the brain.
When your brain is bombarded with this artificial light, it refuses to produce melatonin, the hormone required to initiate the sleep cycle. You are essentially telling your 200,000-year-old software that you are currently standing in the middle of a beach in Ibiza at midday. Then, you lay in the dark and wonder why you are “staring at the ceiling counting regrets” and thinking about that embarrassing thing you said in 2014. You have created a catastrophic biological mismatch between your environment and your evolutionary needs. You are trying to sleep in a world you’ve convinced your brain is perpetual daylight.
7. The Alcohol Myth: The “Drunk Builder” in Your Brain
There is a persistent, stubborn myth that a glass of wine or a stiff nightcap helps with sleep. This is perhaps the most damaging “hack” in our modern repertoire. Let us be clear: alcohol does not help you sleep. It sedates you.
While alcohol might help you “pass out” faster by suppressing the central nervous system, the quality of the ensuing unconsciousness is abysmal. Alcohol is a powerful disruptor of REM (Rapid Eye Movement) sleep, the stage of sleep responsible for emotional processing, memory consolidation, and cognitive health.
“Alcohol does not help you sleep. It sedates you. It knocks you unconscious and then smashes your REM cycles like a drunk builder with a sledgehammer. You wake up feeling like you have been emotionally mugged.”
This is why, after a night of “relaxing” drinks, you wake up feeling fragmented, anxious, and cognitively sluggish. You have bypassed the restorative phases of sleep and replaced them with a state of chemical sedation. You haven’t recovered; you’ve just been put under. The “drunk builder” has spent the night destroying the very architecture your brain needs to function the next day.
8. Caffeine Courage: Mortgaging the Nervous System
Similarly, we use caffeine to mask the symptoms of our self-inflicted sleep debt. That 3 pm coffee is often viewed as a necessary “boost” to get through the final hours of the workday. In reality, that caffeine is “Caffeine Courage”—a false sense of energy that is actually being borrowed from your midnight rest.
Caffeine has a surprisingly long half-life. If you have a coffee at 4 pm, half of that caffeine is still circulating in your brain at 10 pm, blocking the adenosine receptors that signal sleepiness. You are mortgaging your nervous system. You might get a “slightly faster spreadsheet” at 4 pm, but you are ensuring that your nervous system remains in a state of high alert when it should be winding down. You are sacrificing the long-term health of your brain for a short-term illusion of productivity. It is a bad trade, made by people who have forgotten what it feels like to be naturally awake.
9. Silencing the Inner PR Firm: The Psychology of the Midnight Scroll
At approximately 11:17 pm, most of us encounter a very specific, very persuasive internal voice. It is a smooth-talking, silver-tongued entity that says things like:
“Just one more episode of this show, you’re finally relaxing.”
“One more scroll through the news feed; you need to stay informed.”
“You’ve worked so hard today; you deserve this ‘me time’.”
This is your “Inner PR Firm.” It is not your rational self; it is a psychological mechanism designed to sell you tomorrow’s misery at a discount price tonight. It frames self-destructive behaviour as “self-care.” It tells you that staying up until 1 am looking at memes is a reward for a hard day, when in reality, it is a punishment for your future self.
To reclaim your sleep, you must learn the “behavioural coaching” technique of observing and naming this voice. When it starts its pitch at 11:17 pm, stop and say to yourself: “Ah, there’s the Inner PR Firm trying to ruin my Tuesday.” Observe it. Name it. Laugh at the ridiculousness of its arguments. Then, put the phone down like an adult who understands that actions have consequences. The Inner PR Firm does not care about your brain fog, your irritability, or your cravings tomorrow morning; it only cares about the immediate, cheap hit of dopamine. Managing this voice is the first step in returning to a functional, high-integrity human state.
10. The Warrior Sleep Track: Returning to Factory Settings
Fixing your sleep does not require a £300 gadget, a designer supplement, or a subscription to a biohacking app. It requires a return to “factory settings”—the default human mode that your biology expects and demands. These are “no-gadget” solutions that are boring, unglamorous, highly effective, and as fundamental to your health as brushing your teeth.
Morning Light Exposure: Within 30 minutes of waking, get actual daylight in your eyes. This means going outside. Do not look through a window (which filters out the necessary blue-light spectrum); do not wear sunglasses. This light signal acts as a “factory reboot” for the suprachiasmatic nucleus—the master clock in your brain—setting the timer for melatonin production fourteen hours later.
Evening Lighting Environment: After 9 pm, cut all overhead lights. Switch to lamps with warm, low-wattage bulbs. Darkness is the operating environment your brain requires to begin the wind-down process. Stop “interrogating” your brain with Ibiza-style kitchen lighting. Create a sanctuary of shadow.
Cold Water Exposure: End your morning shower with 60 seconds of cold water. It is unpleasant. It is shocking. But it provides a necessary stimulus for the nervous system and helps regulate your body’s thermal rhythm. As the saying goes, “Choose your discomfort.” The short-term discomfort of cold water is infinitely preferable to the decade-long discomfort of chronic, soul-crushing exhaustion.
Nutritional Stability: Eat a high-protein, high-fat breakfast instead of sugar and refined carbohydrates. Stable fuel in the morning leads to a stable blood sugar level throughout the day. This drastically reduces the likelihood of those “9 pm biscuit negotiations” because your biochemistry isn’t on a sugar-induced rollercoaster.
Rigid Consistency: Go to bed and wake up at the same time every day, even on weekends. This is the “brushing your teeth” of sleep health. It isn’t exciting, and it won’t make for a great Instagram post, but it is the foundation of a stable biological system. Your body craves rhythm, not “hacks.”
11. Conclusion: Wiping the Fogged-up Windscreen
When you stop tracking and start actually sleeping, everything in your life becomes markedly easier. Living with chronic sleep debt is like trying to drive a car through a heavily fogged-up windscreen. You are squinting, straining, and constantly on the verge of making a catastrophic mistake. You think the problem is the road, the car, or your driving skills, but the problem is simply that you cannot see.
Fixing your sleep wipes that windscreen clean. Suddenly, the world comes into focus.
Cravings drop because your hormones are no longer feral.
Mood stabilises because your prefrontal cortex is back in charge of your emotions.
Fat loss becomes a natural side effect of a healthy metabolism rather than a constant, losing war of willpower.
Focus and patience return to your work and your relationships.
You stop needing five cups of coffee and a motivational speech just to function at a baseline level. You do not need another tracker to tell you that you’re tired. You do not need another app to tell you to breathe. You do not need another powdered miracle from a “health” influencer.
What you need is darkness, consistency, and the courage to treat your rest as if it is actually important. Because it is the foundation of everything you are. Stop tracking. Start sleeping. Reset the system. What could you achieve if you finally stopped fighting your biology and started working with it?
The Emotional Mastery book is a practical manual for understanding and regulating the human nervous system using the Emotional Operating System framework.
Instead of analysing emotions or retelling your past, the Emotional Mastery book teaches you how to read emotional states as system feedback, identify overload, and restore stability under pressure.
No labels. No therapy-speak. No endless healing loops. Just a clear, operational approach to emotional regulation that actually holds when life applies load.
Emotional Outsourcing, It is 6:00 PM on a Tuesday. You have just walked through the door—or perhaps, given the modern hybrid landscape, you have simply closed a laptop lid on the kitchen table. The house is loud, or perhaps it is deafeningly silent. The transition from “worker” to “parent,” or “employee” to “human,” is jarring. Your shoulders are hovering somewhere around your earlobes. Your jaw is clenched tight enough to crack a walnut.
You walk to the fridge. You take out the bottle. You pour the glass.
And then, the exhale.
That first sip isn’t really about the taste of the Sauvignon Blanc or the craft IPA. It is a biological signal. It is a chemical handshake with your nervous system that says, “Okay, you can stand down now. The danger has passed. The noise can stop.”
We call this “unwinding.” We call it a “nightcap.” We joke about “Wine O’Clock” in socially acceptable memes that plaster social media feeds. But if we are going to be brutally honest with ourselves—and honesty is the only currency that matters here—we need to relabel this behaviour.
You are outsourcing your emotional regulation to a bottle.
This sounds harsh. It sounds like an accusation. But please hear this: this article is not here to shame you. We have enough shame. We have an internal voice—let’s call him BOB (we will meet him properly later)—who handles the shaming department quite effectively on his own.
This article is here to validate you. Because the reason you are outsourcing your regulation to a bottle isn’t because you are weak, or an addict, or morally failing. It is because you are being asked to endure unmanageable levels of stress, stimulation, and emotional labour without support.
That is where the system breaks. And that is the part nobody wants to look at yet.
In this comprehensive guide, we are going to dismantle the mechanics of why we drink to cope, explore the devastating concept of “unsupported endurance,” and introduce a new framework—the Emotional Observation Method (EOM)—to help you reclaim the controls of your own operating system.
PART 1: The Mechanics of Outsourcing Regulation
To understand why we outsource regulation, we first must understand what regulation actually is.
Emotional Regulationis the ability of the nervous system to navigate the waves of human experience—stress, joy, anger, fear—and return to a baseline state of safety and equilibrium. When we are regulated, we can handle a difficult email from a boss without spiralling. We can deal with a toddler’s tantrum without screaming back. We remain within our “Window of Tolerance.”
However, modern life rarely keeps us in that window. Modern life is a relentless assault on the nervous system. The notifications never stop. The demands for productivity are infinite. The cost of living crisis, the geopolitical instability, the personal traumas—it is a constant bath of cortisol and adrenaline.
The Chemistry of the “Quick Fix”
When your nervous system is stuck in “Fight or Flight” (Sympathetic activation) for 10, 12, or 14 hours a day, it forgets how to downshift. You are revving the engine in neutral. You cannot simply “decide” to relax. The physiological momentum is too strong.
Enter alcohol.
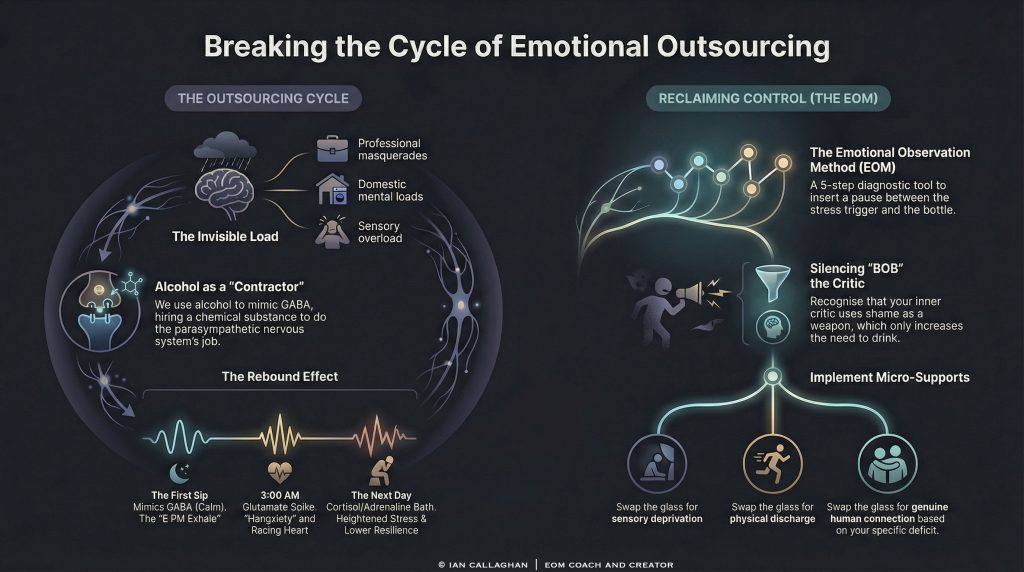
Alcohol is a central nervous system depressant. It mimics GABA (gamma-aminobutyric acid), the neurotransmitter responsible for calming neuronal activity. When you drink, you are essentially flooding your brain with synthetic “calm down” juice. It forces the brakes on your revving engine.
This is why it feels so effective. It works fast. It is reliable. It is accessible.
When you pour that glass, you are saying to your body: “I do not have the internal resources, the time, or the support to regulate this stress naturally. So, I am hiring a contractor to do it for me.”
You are outsourcing the job of the parasympathetic nervous system to a substance.
The Problem with Outsourcing
If you outsourced your job to someone who did it quickly but damaged the office every time they visited, you would eventually fire them. Alcohol is that destructive contractor.
While it provides immediate relief (regulation), it creates a rebound effect. As the alcohol wears off, the brain realises it has too much GABA and not enough glutamate (the excitatory neurotransmitter). To compensate, it spikes your anxiety levels the next day. This is the “hangxiety” or the 3:00 AM wake-up call where your heart is racing and BOB is screaming at you about everything you did wrong in 1999.
This creates a cycle:
Endure high stress without support.
Outsource regulation to the bottle to survive the evening.
Experience heightened anxiety and lower resilience the next day due to the chemical rebound.
Endure even harder to compensate for the fatigue.
Repeat.
But to break this cycle, we cannot just “stop drinking.” That is a surface-level fix. We have to look at why the regulation is needed in such desperate quantities in the first place.
PART 2: What Are You Enduring? (The Invisible Load)
The most critical sentence in our premise is this: “…start noticing what you’re being asked to endure without support.”
Society loves to talk about “burnout,” but it treats burnout as an individual failure of time management or self-care. It suggests that if you just journaled more, did more yoga, or drank more green juice, you wouldn’t be burnt out.
This is a lie.
You are likely drinking because you are enduring the unendurable. You are carrying loads that human beings were not evolved to carry, in isolation that human beings were not evolved to experience.
The Museum of Endurance
Let us walk through the gallery of modern endurance. Look closely, and see if you recognise yourself in these exhibits.
1. The Professional Masquerade You are expected to perform at peak cognitive capacity for 8 to 10 hours a day. But it is not just the work; it is the performance of work. It is the emotional labour of navigating office politics, the “always-on” Slack culture, and the unspoken expectation that you must be grateful for your exploitation. You are enduring the suppression of your true self to fit a corporate mould.
2. The Domestic CEO If you are managing a household, you are the Chief Logistics Officer, the Chief Financial Officer, the Head of Conflict Resolution, and the Sanitation Department. The “mental load”—remembering birthdays, scheduling dentist appointments, noticing we are out of milk—is a ticker tape that never stops running in your mind. You are enduring a level of cognitive multitasking that would crash a computer.
3. The Sensory Overload We live in an attention economy. Your phone is designed to hijack your dopamine receptors. The news cycle is a 24-hour stream of catastrophe. You are enduring a level of sensory input that keeps your amygdala (the threat detection centre) permanently activated.
4. The Isolation Tank This is the “without support” part. We live in nuclear families or single-person households, separated from the “village” structures we evolved in. When you are struggling, who holds you? Who regulates the regulator? Often, the answer is “nobody.” You are the rock for everyone else.
When you combine these factors, the glass of wine is not a beverage. It is an anaesthetic. It is the only way to numb the pain of endurance so you can get up and do it again tomorrow.
PART 3: Meet BOB (The Inner Critic)
We cannot talk about this cycle without introducing the loudest voice in the room: BOB.
BOB is your Inner Critic. He is that nagging, sneering, relentless voice in your head. He has a lot to say about your outsourcing habits.
When you reach for the bottle, BOB says:
“Look at you. Can’t even handle a Tuesday without a drink.”
“You’re turning into your father/mother.”
“You’re weak. Everyone else is coping fine. Why can’t you?”
BOB loves to use shame as a weapon. He believes that if he beats you up enough, you will shape up. He thinks shame is a motivator.
But here is the truth about BOB: He is actually trying to protect you.
It sounds counterintuitive, but BOB is a primitive part of your psyche. He is terrified of social rejection. In our tribal past, being “weak” or “lazy” or “addicted” meant you might be cast out of the tribe, which meant death. So, BOB screams at you to try to force you into compliance with societal standards.
The problem is, BOB is outdated. He is running on legacy software. He doesn’t understand that the “threat” isn’t a sabre-toothed tiger; the threat is late-stage capitalism and a lack of community care.
When BOB shames you for drinking, he actually increases your stress levels. Increased stress requires more regulation. Since you don’t have natural support, you reach for the bottle again.
BOB is fueling the very fire he is screaming at you to put out.
We need to stop fighting BOB and start understanding him. We need to say, “Thank you for your concern, BOB, but I am handling this differently now. I am going to use the EOM.”
PART 4: The Void of Support – Where It Actually Breaks
“That’s where this actually breaks. And that’s the part nobody wants to look at yet.”
Why does nobody want to look at it? Because looking at it requires admitting that our current way of living is structurally unsound.
If we admit that we are drinking not because we love the taste of Pinot Grigio, but because we are lonely, overworked, and terrified, we have to demand change. We have to demand better childcare. We have to demand reasonable working hours. We have to demand men take on equal emotional labour. We have to demand communities that care for each other.
That is a revolution. Drinking is sedition.
When you outsource regulation to a bottle, you are engaging in a private act of survival that prevents a public act of change. As long as we can numb ourselves enough to get through the week, the system doesn’t have to change.
But the personal cost is too high. You are paying for this “stability” with your health, your connection to yourself, and your authentic joy.
The “Strong One” Syndrome
Many of us who rely on this mechanism identify as “The Strong One.” We are the ones people come to for advice. We are the ones who don’t crack.
Enduring without support is a badge of honour for The Strong One. But inside, The Strong One is crumbling. The bottle is the only place where The Strong One allows themselves to be “soft,” even if that softness is chemically induced.
Recognising this is painful. It requires grieving. It requires grieving the fact that you have been neglected—perhaps by society, perhaps by a partner, perhaps by your family of origin.
You have been asked to carry a mountain. It is not your fault that your legs are shaking. It is not your fault that you grabbed a crutch.
But now that we see the crutch for what it is, we can start to build real muscle.
PART 5: The Solution – The Emotional Observation Method (EOM)
If we are to stop outsourcing regulation to a bottle, we must bring the regulation in-house. We must install a new protocol.
We are not talking about “positive thinking” or “willpower.” Those are finite resources. We are talking about the Emotional Observation Method (EOM).
Clarification: The EOM is not your emotional operating system. Your operating system is the complex web of trauma responses, beliefs, and neural pathways you currently run on. The EOM is the tool or the technique we use to work on that operating system. Think of it as the diagnostic software and the repair kit combined.
The goal of EOM is to insert a pause between the Trigger (Stress/Endurance) and the Response (The Bottle).
Step 1: The Pause (Interrupting the Pattern)
The moment you feel the urge to drink—that 6:00 PM itch—is data. It is not a command; it is information.
Instead of autopiloting to the fridge, you must physically stop. Sit down for 60 seconds.
Step 2: Locate the Sensation
Get out of your head (where BOB lives) and into your body. What does the urge feel like somatically?
Is it a tightness in the chest?
A buzzing in the hands?
A hollow pit in the stomach?
A frantic energy behind the eyes?
Name the sensation. “I am noticing a tightness in my throat.”
Step 3: Identify the Deficit (The “Without Support” Check)
Ask yourself: “What am I actually trying to regulate right now?”
Do not accept “I just want a drink” as an answer. Dig deeper.
“I am trying to regulate the anger I feel about that meeting.”
“I am trying to regulate the loneliness I feel in this empty house.”
“I am trying to regulate the exhaustion of pretending to be okay.”
This is the hardest part. This is where you acknowledge what you have been enduring without support.
Step 4: Validate the Need
Speak to yourself (or to BOB) with radical compassion. “It makes total sense that I want a drink right now. I have been holding it together for 10 hours. I am exhausted and I feel unsupported. My body is screaming for relief.”
This validation drops the shame. When shame drops, the cortisol spikes lower, and the urgency often decreases.
Step 5: The Micro-Support Choice
If the root cause is “enduring without support,” the solution is to provide support. Since we cannot instantly summon a village or change society, we must provide Micro-Support to ourselves.
If you are:
Overstimulated: You need sensory deprivation. Go into a dark room, put on noise-cancelling headphones, and lie on the floor for 10 minutes. (This regulates the nervous system better than wine).
Angry/Frustrated: You need a sympathetic release. Scream into a pillow. Punch a mattress. Shake your body vigorously to discharge the adrenaline.
Lonely: You need connection. Call a friend (and tell them the truth, not the highlight reel). Hug a pet. Or simply place your hand on your heart and breathe.
Exhausted: You need rest. Not “numbing out” in front of Netflix, but actual rest. A hot bath. Yin yoga. Sleep.
The EOM doesn’t say you can’t have the drink. It just asks you to perform this diagnostic first. Often, once you have identified the emotion and offered a micro-support, the desperate need for the bottle dissipates. You might still have a glass, but you are drinking it to enjoy it, not to survive yourself.
PART 6: Building Infrastructure for the Future
The EOM helps in the moment. But to truly stop the cycle of endurance, we need structural change in your life.
1. Resigning as General Manager of the Universe
You must look at what you are enduring and start saying “No.” If you are doing the work of three people, you must stop. This is terrifying. BOB will scream, “If I don’t do it, it won’t get done!” Let it not get done. Let the laundry pile up. Let the email wait. If the only way the system works is by you breaking yourself to fuel it, the system deserves to break. You are not a load-bearing wall for everyone else’s comfort.
2. Recruiting Support
You need to stop “outsourcing to a bottle” and start “outsourcing to humans.” This means being vulnerable. It means telling your partner, “I am drowning, and if I don’t get help, I am going to break.” It means looking for a therapist, a men’s group, a women’s circle, or a community organisation. It means realising that independence is a trauma response, and interdependence is the goal.
3. Rewiring the Reward System
Your brain has associated alcohol with the “End of Shift.” You need new rituals to signal safety to your body.
Change your clothes immediately upon finishing work.
Take a shower (water is a great state-changer).
Go for a walk around the block to physically separate “work” from “home.”
Brew a complex herbal tea (the ritual of preparation matters).
PART 7: A Note on “The Part Nobody Wants to Look At”
We must circle back to the profound truth of the prompt: “That’s the part nobody wants to look at yet.”
When you stop numbing yourself, you start feeling. And initially, that feeling might be rage. You might look at your marriage and realise it is empty. You might look at your job and realise it is exploitative. You might look at your past and realise you were neglected.
Alcohol was the fog that kept these sharp edges hidden. When the fog lifts, the edges cut. This is why sobriety (or mindful drinking) is so incredibly difficult. It is not just about the substance; it is about facing the reality of your life without a filter.
But this is also where the magic happens. Because you cannot change what you cannot see. As long as you are outsourcing regulation, you are maintaining the status quo. When you stop, and you feel the rage, the grief, and the exhaustion, you finally generate the energy required to change your life.
You stop enduring. You start living.
Conclusion: From Endurance to Experience
You do not need another glass of wine. You need a hug. You need a break. You need to be heard. You need to know that you are not a machine designed for endless output.
The bottle is a liar. It promises connection but delivers isolation. It promises relaxation but delivers anxiety. It promises to help you carry the load, but it only makes the load heavier tomorrow.
By using the Emotional Observation Method, and by courageously facing BOB, you can begin to dismantle the architecture of endurance that has trapped you.
It is time to stop outsourcing your regulation. It is time to bring the operations back in-house. It will be messy. It will be loud. You will feel things you haven’t felt in years.
But you will be free. And you will be supported—first by yourself, and then, slowly, by the authentic connections you build when you stop hiding behind the glass.
You are worth more than what you can endure. Start there.
The Emotional Mastery book is a practical manual for understanding and regulating the human nervous system using the Emotional Operating System framework.
Instead of analysing emotions or retelling your past, the Emotional Mastery book teaches you how to read emotional states as system feedback, identify overload, and restore stability under pressure.
No labels. No therapy-speak. No endless healing loops. Just a clear, operational approach to emotional regulation that actually holds when life applies load.
The Toxicology of Alcohol: Why It’d Be Banned in 2026
The only reason alcohol is legal in the UK or the US today is a historical accident. If a pharmaceutical company tried to bring “Ethanol” to the market in 2026 as a new recreational substance, it would fail every safety trial, every MHRA standard, and every FDA review immediately. It wouldn’t even make it past the preliminary toxicology report.
I spent 45 years drinking. I’ve lived in the trenches of the British pub culture and the military drinking tradition. But as a qualified nutrition expert with deep roots in biochemistry and human physiology, I have to be brutally clear: Alcohol is a neurotoxic carcinogen. We have been socially engineered to call it “tradition,” but your cells recognise it only as a systemic crisis. This is not a moral argument; it is a chemical one.
The Regulatory Rejection: Alcohol vs. Modern Standards
If a regulatory body like the MHRA (Medicines and Healthcare products Regulatory Agency) were to review alcohol today, the application would be denied before the first coffee break. To understand why, we have to look at the clinical profile of the molecule itself—not the marketing, not the craft labels, and not the “sophisticated” wine culture we’ve built around it.
The Toxicity Profile (LD50) and Therapeutic Index
Every substance in toxicology is measured by its LD50—the dose required to kill half a tested population. Ethanol has a remarkably narrow therapeutic index. In many cases, the gap between a “recreational” dose and a lethal one is less than a factor of ten. Compare this to modern regulated substances or even “natural” medicines, and alcohol looks like weapons-grade poison.
In a modern laboratory setting, a substance with such a high potential for acute overdose, combined with its long-term organ toxicity, would be classified as a high-risk poison. If we invented a drink today where “three or four times the social dose” could lead to respiratory failure, coma, and death, it would never reach a supermarket shelf. It would be kept behind a pharmacy counter or, more likely, banned entirely for recreational use.
1. The Group 1 Carcinogen Reality
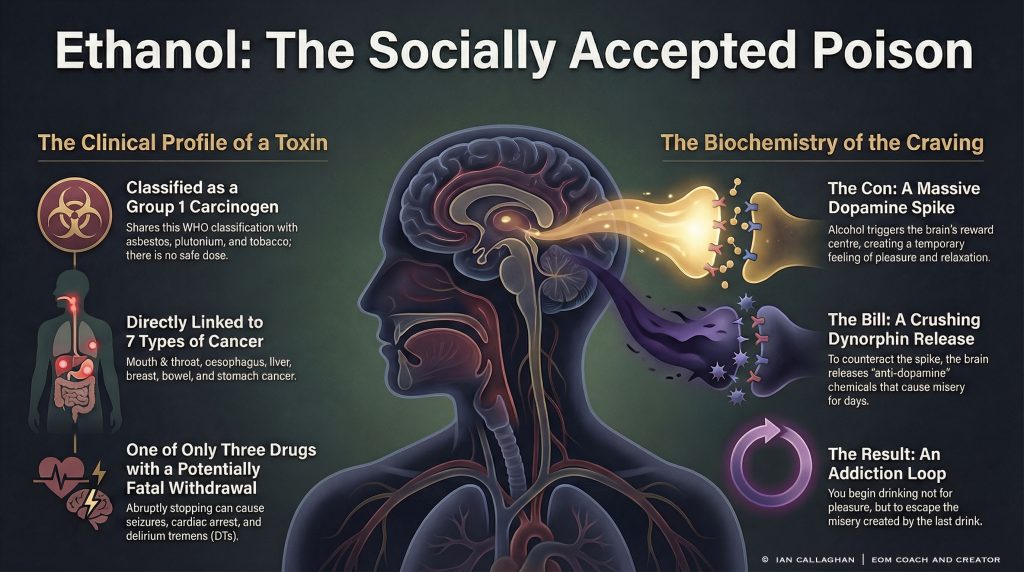
Alcohol sits in the same World Health Organisation (WHO) category as asbestos, plutonium, and tobacco. This isn’t a “judgment call” or “anti-booze propaganda.” It is a classification based on undisputed, peer-reviewed toxicology.
There is no “safe dose” when it comes to DNA damage. When you consume ethanol, your body immediately prioritises its breakdown because it cannot store it. The primary metabolite is acetaldehyde—a highly reactive chemical that is a proven mutagen.
How Acetaldehyde Destroys Your DNA
Acetaldehyde is up to 30 times more toxic than ethanol itself. It literally breaks your DNA strands, causes cross-linking (where the two strands of the DNA double helix are permanently stuck together), and prevents your body from repairing the damage. When DNA repair fails, the cell either dies or mutates. Mutation is the gateway to cancer.
This chemical assault leads directly to seven primary types of cancer:
Mouth and Throat: The first points of contact. Ethanol acts as a solvent, making the delicate mucosal membranes more permeable to other carcinogens, such as those found in tobacco or processed foods.
Oesophagus: Chronic irritation and the constant presence of acetaldehyde lead to cellular mutation of the lining.
Liver: This is “Ground Zero.” As the liverLiveresses the toxin, it generates massive oxidative stress. This leads to Steatosis (fatty Liver), Fibrosis (scarring), then Cirrhosis (permanent death of liver tissue), and finally Hepatocellular Carcinoma (liver cancer).
Breast: Alcohol increases levels of estrogen and other hormones associated with hormone-receptor-positive breast cancer. It also decreases the body’s ability to absorb essential nutrients that protect against cell damage, such as folate.
Bowel and Stomach: Constant inflammation of the digestive tract and the total disruption of the microbiome—the “Leaky Gut” effect—allows carcinogenic byproducts to enter the bloodstream, creating a pro-cancer environment throughout the body.
The Fatal Withdrawal Paradox: A Regulatory Red Flag
In the world of drug regulation, the “Danger Profile” of a substance is often measured by its withdrawal mechanics. There are only three common substances where the withdrawal itself can kill you: Benzodiazepines, Barbiturates, and Alcohol. Even Opioid withdrawal, as agonising as it is, rarely stops the heart. Alcohol withdrawal is a medical emergency because of a phenomenon called Excitotoxicity.
The GABA/Glutamate War: The Brain Under Siege
Alcohol is a central nervous system depressant. It works by mimicking GABA, your brain’s primary inhibitory neurotransmitter (the “brake”). To counter this constant suppression, the brain increases glutamate production, the primary excitatory neurotransmitter (the “gas”).
When you drink for years, your brain is essentially driving with one foot slammed on the brake and the other slammed on the gas. When you suddenly remove the alcohol, the “brake” is gone, but the “gas” is still floored. This leads to a massive, toxic surge of Glutamate:
Seizures: The brain’s electrical system short-circuits from over-excitation.
Delirium Tremens (DTs): A state of extreme confusion, hallucinations, and tremors.
Cardiac Arrest: The heart’s electrical system is overwhelmed by the chemical surge, leading to sudden death.
If we invented a drink today that could kill you simply because you stopped drinking it, it would be labelled a high-risk controlled substance within 24 hours. The fact that it is available in every corner shop is a testament to historical momentum, not public safety.
Systematic Solvent Damage: The “Whole Body” Hit
Ethanol is a “solvent.” It is both water and fat-soluble, meaning it permeates every single cell in your body. It doesn’t “pass through” you; it integrates into your biology and destroys it from the inside out.
Neurotoxicity and the Blood-Brain Barrier
Alcohol crosses the blood-brain barrier with ease. Once inside, it acts as a neurotoxin, physically shrinking the brain’sgreyy matter. Over decades of drinking, this leads to:
The Lobotomized Prefrontal Cortex: The part of the brain responsible for impulse control, long-term planning, and social behaviour. Alcohol “turns off” this section first, which is why your “Zero Fucks” button gets stuck when you’re drunk.
Amygdala Hijack: Alcohol increases the sensitivity of the amygdala, the brain’s fear centre. This is why long-term drinkers often suffer from chronic anxiety and paranoia when they aren’t drinking.
Wernicke-Korsakoff Syndrome: Also known as “Wet Brain,” this is a permanent form of dementia caused by thiamine (Vitamin B1) deficiency, which alcohol directly causes by blocking absorption in the gut.
Cardiomyopathy and the “Holiday Heart”
The “heart-healthy” myth of red wine was one of the greatest marketing cons of the 20th century. Ethanol is directly toxic to the heart muscle (myocardium). It leads to alcoholic cardiomyopathy, where the heart weakens and thins, unable to pump blood efficiently. It also spikes blood pressure and triggers arrhythmias like Atrial Fibrillation (often called “Holiday Heart Syndrome”). Chronic drinkers are essentially walking around with an engine that misfires and leaks oil.
Mitochondrial Collapse and the ATP Crisis
As a nutrition expert, I focus on the mitochondria—the engines of your cells. Every cell in your body needs ATP (energy) to function. Alcohol is a “metabolic priority.” Your body cannot store ethanol, so it halts all other functions, including fat burning and nutrient absorption, to deal with the chemical fire.
This causes a massive surge in Reactive Oxygen Species (ROS), effectively “rusting” your cells. When your mitochondria fail, your energy fails. You aren’t just “tired”; your cells are literally running out of the currency they need to stay alive. This is why hangovers feel like a near-death experience—because, at a cellular level, they are.
The Biochemistry of Desire: The Science of the Craving
Most people think a craving is a “lack of willpower.” It isn’t. A craving is a biological mandate issued by a hijacked nervous system. To understand why you can’t “just have one,” you have to understand the Dopamine-Dynorphin Seesaw.
The Dopamine Spike (The Con)
When ethanol hits your system, it triggers a massive release of dopamine in the nucleus accumbens—the brain’s reward centre. This is the “Aha!” moment. It feels like relaxation or confidence. But because alcohol is a depressant, the brain has to maintain homeostasis. It cannot let you stay that high forever, or your system would collapse.
The Dynorphin Crash (The Bill)
To counter the massive dopamine spike, your brain releases Dynorphins. Think of Dynorphins as “anti-dopamine.” They are the chemicals of misery, restlessness, and discontent. They turn down the volume on your joy so that the alcohol doesn’t overstimulate you.
The problem? Dopamine leaves the system in minutes. Dynorphins stay for days.
This is why, at 3:00 AM after a night of drinking, you wake up with “The Horrors.” That isn’t just guilt; it’s the Dynorphins making you feel physically and emotionally wretched. Your brain then tells you the only way to get rid of that feeling is another spike of dopamine. This is the “Loop.” You aren’t drinking for pleasure anymore; you are drinking to neutralize the misery created by the last drink. This is the Chemical Hijack.
The Quartet of Destruction: Alcohol, Sugar, Seed Oils, and Wheat
If you want to understand why you feel like shit even when you aren’t drinking, you have to look at the Quartet of Destruction. Alcohol is rarely the only toxin in the system.
1. Alcohol: The Lead Toxin
The primary neurotoxin that stops fat-burning, inflames the gut, and damages DNA. It is the “entry drug” for metabolic syndrome and type 2 diabetes.
2. Refined Sugar: The Dopamine Mirror
Alcohol is effectively a liquid sugar delivery system. When you remove the ethanol, your brain still wants that massive dopamine hit, and it knows that refined sugar is the closest legal equivalent. If you swap the bottle for the biscuit tin, you aren’t healing; you’re just shifting the dependency.
3. Seed Oils: The “Double Hit” to the Liver
Industrial vegetable oils (Soybean, Corn, Canola) are high in Linoleic Acid, an Omega-6 fatty acid that is highly unstable. When you combine Seed Oils with Alcohol, you create a “Double Hit” to the Liver.
Alcohol increases gut permeability (Leaky Gut), allowing endotoxins from your bacteria to enter the Liver, while the seed oils have already created a pro-inflammatory environment. Research suggests that this combination accelerates Cirrhosis significantly faster than alcohol alone. If you’re drinking wine and eating “healthy” stir-fries cooked in rapeseed oil, you are still poisoning your Liver.
4. Wheat/Gluten: The Gut Permeability Factor
Wheat contains Zonulin, a protein that regulates the “tight junctions” in your gut lining. Modern wheat and alcohol both increase Zonulin, leading to a permanent state of Leaky Gut. This allows undigested food particles and bacteria to enter the bloodstream, triggering a systemic immune response. Your brain fog isn’t just the booze; it’s the immune system attack caused by your “standard” diet.
As a nutrition expert, I don’t just tell people to “stop drinking.” I tell them to stop the biological napalm. You cannot heal a liver that is being bombarded by alcohol and inflammatory seed oils simultaneously.
Why Is It Still Legal? The “Grandfather” Loophole
If alcohol is so toxic, why is it next to the bread in Sainsbury’s? Why do we advertise it during the football and pour it at christenings? The answer isn’t “safety”—it’s history, revenue, and conditioning.
The Treasury Factor: Governments as Pushers
In the UK, alcohol generates roughly £12 billion in yearly tax revenue. In the US, the numbers are even more staggering. Governments are effectively “addicted” to the revenue generated by a substance that costs the healthcare system nearly double that amount in related illnesses, violence, and policing. They aren’t going to ban it because they can’t afford the withdrawal symptoms in their own budgets.
The “Culture” Shield: Marketing the Poison
We have been conditioned to associate wine with “sophistication” and beer with “mateship.” We use these labels to hide the molecule. We call it “spirit,” “craft,” or “vintage” to distract ourselves from the fact that it is ethanol—the same stuff we put in petrol tanks. The alcohol industry spends billions ensuring that you view your dependency as a “lifestyle choice” rather than a toxicological reality.
Normalised Poisoning: The Peer Pressure Machine
We are the only society that mocks people for not consuming a Group 1 carcinogen at a weekend party. If you turned down a cigarette, no one would call you “boring.” If you turned down a neurotoxin, and suddenly you’re the “odd one out.” This social engineering is designed to keep you in the loop, because as long as everyone else is drinking, no one has to look at the bill.
Reclaiming Your Operating System: The EOM Method
If you have spent 45 years—or even 5 years—running on this toxic fuel, your “Emotional Operating System” (EOS) is glitchy. You drink to numb the noise, but the drink is what creates the noise in the first place.
Step 1: Identify the Loop
Most drinking is “maladaptive regulation.” You are trying to calm a nervous system that alcohol has already fried. You have to stop viewing the drink as the solution and start viewing it as the source of the fire.
Step 2: The Physical Reset (Autophagy)
You cannot fix the mind while the body is under chemical siege. This is why my approach focuses on Autophagy—the body’s natural “cell autophagy” mechanism. By removing toxins (Alcohol, Sugar, Seed Oils, Wheat) and using protocols like Intermittent Fasting, we trigger the body to break down damaged cells and mitochondria and replace them with new, high-performance ones. You have to clear the metabolic fog before you can rewire the hardware.
Step 3: Emotional Observation Method (EOM)
Once the toxin is gone, the emotions return at full volume. You need a mechanical framework to “Observe” these states without reacting to them. This is how you transition from “white-knuckling it” to true emotional mastery. You stop “being” the emotion and start “observing” the data.
FAQ: The Hard Truths (What They Don’t Tell You in the Pub)
Q: Is “moderation” actually a healthy goal?
A: Moderation is a term invented by the alcohol industry to keep you “functionally addicted.” From a purely toxicological standpoint, there is no “healthy” amount of a Group 1 carcinogen. You are simply poisoning yourself more slowly.
Q: How long does it take for the liver to heal?
A: The liver is the only organ that can fully regenerate, but it needs a total cessation of the toxin. Through a strict nutritional protocol that reduces inflammation and supports autophagy, a significant improvement in liver enzymes (ALT/AST) within 30 to 90 days.
Q: Why do I feel bored when I stop?
A: Because your dopamine receptors are fried. They’ve been blasted by “weapons-grade” stimulation for years. It takes about 90 to 120 days for your brain to start finding “normal” things—like a sunset or a conversation—interesting again. This is a chemical recalibration, not a character flaw.
Q: What is acetaldehyde exactly?
A: Acetaldehyde is the first byproduct of ethanol metabolism. It is up to 30 times more toxic than alcohol itself. It is a known carcinogen that causes DNA cross-linking, which leads to permanent genetic mutations and cancer. It is the reason for the “hangover” and the long-term damage.
Q: Can I repair my mitochondria?
A: Yes. Through a combination of removing toxins, strength training, and cold exposure, you can trigger Mitochondrial Biogenesis—the creation of new, healthy power plants in your cells.
FEATURED PRODUCT
Emotional Mastery: The Emotional Operating System
The Essential Toolkit for Reclaiming Your Life.
If you are struggling with the science of cravings or the emotional “Freight Train” described in this report, you need a mechanical framework to manage your system.
Stop the Loop: Identify triggers before they hijack you.
Rewire the Response: Practical Tools for Real-World Stress.
Veteran-Led: No fluff, just the method I used after 45 years of drinking.
Stop doing the social wilderness alone. Join 5,000+ veterans and high-performers who are using the EOM method to reclaim their lives. Get daily support, live Q&As, and a community that actually “gets it.”
Ian Callaghan is a veteran, a sobriety coach, and a nutrition expert. After 45 years of drinking, he used his background in biochemistry and the EOM method to engineer his own “Reset.” He now helps over 37,000 followers navigate the brutal reality of reclaiming their lives through physical resets and emotional mastery.
The Emotional Mastery book is a practical manual for understanding and regulating the human nervous system using the Emotional Operating System framework.
Instead of analysing emotions or retelling your past, the Emotional Mastery book teaches you how to read emotional states as system feedback, identify overload, and restore stability under pressure.
No labels. No therapy-speak. No endless healing loops. Just a clear, operational approach to emotional regulation that actually holds when life applies load.
Used to monitor number of Google Analytics server requests when using Google Tag Manager
1 minute
_gid
ID used to identify users for 24 hours after last activity
24 hours
_ga_
ID used to identify users
2 years
_gali
Used by Google Analytics to determine which links on a page are being clicked
30 seconds
_ga
ID used to identify users
2 years
__utmx
Used to determine whether a user is included in an A / B or Multivariate test.
18 months
__utmv
Contains custom information set by the web developer via the _setCustomVar method in Google Analytics. This cookie is updated every time new data is sent to the Google Analytics server.
2 years after last activity
__utmz
Contains information about the traffic source or campaign that directed user to the website. The cookie is set when the GA.js javascript is loaded and updated when data is sent to the Google Anaytics server
6 months after last activity
__utmc
Used only with old Urchin versions of Google Analytics and not with GA.js. Was used to distinguish between new sessions and visits at the end of a session.
End of session (browser)
__utmb
Used to distinguish new sessions and visits. This cookie is set when the GA.js javascript library is loaded and there is no existing __utmb cookie. The cookie is updated every time data is sent to the Google Analytics server.
30 minutes after last activity
__utmt
Used to monitor number of Google Analytics server requests
10 minutes
__utma
ID used to identify users and sessions
2 years after last activity
_gac_
Contains information related to marketing campaigns of the user. These are shared with Google AdWords / Google Ads when the Google Ads and Google Analytics accounts are linked together.