Introduction: The Noise in the Mirror
Step into the digital town square—Instagram, TikTok, or X—and you are immediately met with a polished, high-definition version of “health.” It is a world of ring lights, carefully curated “What I Eat in a Day” montages, and influencers who speak about metabolic health as if it were a trending hashtag rather than a complex biological reality. In this space, the Glucagon-like peptide-1 (GLP-1) receptor agonist has been elevated to the status of a holy relic. It is presented as a “miracle pen,” a frictionless gateway to a thinner, happier life, often accompanied by a discount code and a sunny disposition. For the casual observer, it looks like salvation in a pre-filled syringe.
However, for those who have spent years navigating the gritty reality of chronic weight struggles, this polished narrative feels hollow. There is a profound disconnect between the “influencer” version of weight loss and the lived experience of someone existing in a 20-stone body. The glossy content ignores the “33 amceiling stare”—that quiet, desperate moment when the heart races, the sheets are damp with the sweat of systemic inflammation, and you swear that tomorrow will be the day you finally break the cycle of self-destruction. You wake up with the best of intentions, only to find yourself back in the same “metabolic mess” by lunchtime, defeated by a biological drive you cannot outrun.
We are currently witnessing what can only be described as “The GLP-1 Grift.” This isn’t just about a medication; it is about the predatory industry that has sprung up around it, selling two specific flavours of misinformation: the “Miracle Drug Gospel” and “End-of-the-World Hysteria.” Both extremes serve the interests of those selling a product or a platform, but neither helps the individual make a sane, informed decision about their health. The grifters ignore the nuance because nuance doesn’t go viral.
The reality of metabolic health is rarely found in a sponsored post. It is found in the shame of the “functioning lie,” the hiding of habits, and the hard-earned, messy work of behaviour change. This investigation intends to peel back the influencer perfume and distil the hard truths about GLP-1s that the ring-light educators ignore. We will move beyond the superficial noise to explore why these drugs are a tool, not a transformation, and why using them without rebuilding your “internal operating system” is simply renting results that you will eventually have to return with interest.
2. The Grifter’s Playbook: Miracle Gospel vvsHysteria
The current discourse surrounding GLP-1s is a masterclass in the “Grifter’s Playbook.” On one side, you have the evangelists who frame these injections as “salvation in a pen,” a consequence-free bypass for ananyifestyle efforts. On the other hand, you have the alarmists preaching a gospel of terror, suggesting that these drugs are an existential threat to humanity, designed to bypass the soul and ruin the gut.
Both of these camps are financially motivated. The “miracle” narrative drives private prescriptions and affiliate sales for online pharmacies. In contrast, the “hysteria” narrative drives clicks, engagement, and the sale of alternative “natural” cures that are often just expensive sawdust in a capsule. This cycle is nothing new; it is merely the latest iteration of a long-standing scam that preys on the vulnerable.
“I’ve watched the same cycle play out for years, different product, same scam. First, it was detox teas and ‘cleanse’ packs. Then it was keto zealots screaming that carbs are the devil. Then it was calorie-counting cults telling people they’re morally weak for being hungry. Now it’s GLP-1s.”
In the United Kingdom, this grift has found incredibly fertile ground. According to NHS Digital, approximately 25.9% of adults in England are living with obesity, and a further 37.9% are overweight. With NHS waitlists for specialist weight management services (Tier 3 and Tier 4) reaching a breaking point—often extending to years in certain trusts—thousands of desperate individuals are turning to the private sector. This has given rise to a “Wild West” of metabolic health. Private clinics offer prescriptions via five-minute online questionnaires, bypassing the essential face-to-face medical consultations and psychiatric screening required for such powerful hormonal interventions.
The industry projections are staggering; analysts at Goldman Sachs and JP Morgan suggest the GLP-1 market could reach $100 billion by 2030. This financial incentive ensures that the “Miracle Gospel” remains loud. However, the “Hysteria” camp is just as lucrative, feeding into the UK’s specific brand of health anxiety. Both flavours of bullshit serve to obscure the truth: that for the right person, these are life-changing medical tools, but for the wrong person, they are an expensive way to stay stuck in a cycle of metabolic dysfunction. When the loudest voices in the room have never lived with the physical and emotional burden of metabolic dysfunction, their “opinions” are little more than noise. Honesty in this space is rare because acknowledging that this is hard, messy work doesn’t sell as well as a “miracle.”
3. The Empathy Gap: Why ‘Lived Experience’ Matters
There is a vast “empathy gap” in the weight loss industry. It exists between those who study obesity in a lab or promote it on a screen and those who live it in the flesh. When we talk about a “20 stone body,” we aren’t just talking about a number on a scale; we are talking about a specific type of daily friction. It is the sensory reality of the “metabolic mess”—the physical sensation of systemic inflammation that feels like a low-grade fever, the specific psychological mechanisms of “food noise” that function like a dopaminergic loop you cannot exit.
The “3 am ceiling stare” is the emotional heart of this struggle. This is the hour of the “functioning lie.” Many people struggling with their weight are high performers—doctors, lawyers, executives, parents—who are “functioning” in the eyes of the world but whose private relationship with food is a disaster. They hide their eating habits, disposing of wrappers in outside bins, and they negotiate with their cravings like they are dealing with a hostage-taker. The brain, starving for a dopamine hit to regulate a stressed-out nervous system, bargains for “just one more” until the bag is empty and the shame sets in.
Influencers providing “ring light education” rarely address this shame because it isn’t aesthetic. They treat weight loss as a series of simple choices rather than a deep, psychological rebuild. But lived experience teaches you that metabolic health isn’t just about what you eat; it’s about why the brain demands a “state change” at 9 pm on a Tuesday. The “food noise” isn’t just hunger; it’s an intrusive, non-stop broadcast that overrides logic.
True health is “messy” and “earned.” It involves moving beyond “the hard way” to find structure, standards, and what I call “boring consistency.” When someone who has never felt the overwhelming, irrational drive of a dysregulated metabolism tells a clinically obese person to “just have more willpower,” they are demonstrating a profound lack of understanding. It is like telling someone in a hurricane to “just stand still.” Conversely, when an influencer tells you that a pen is “salvation,” they are ignoring the fact that you still have to live with yourself once the appetite is suppressed. The truth—that these drugs can help quiet the “war” in your head but cannot fix the underlying life that caused the mess—is the only currency worth trading in.
4. Appetite Suppression is Not an Identity Shift
The core mechanism of GLP-1s—mimicking the hormone that tells your brain you are full—is revolutionary for those whose internal signalling is broken. It lowers the “food noise” to a whisper. For many, this provides the first moment of peace they have had in decades. However, as a behavioural change specialist, I must be clear: biological appetite suppression is not the same as psychological behaviour change.
A GLP-1 is a chemical mute button, but it is not “discipline in a pen.” Discipline is an identity-level shift; it is the transition from being a “victim of hunger” to becoming an “architect of health.” If you rely solely on the drug to make your choices, you aren’t actually developing the skill of making decisions. You are simply existing in a state where the decision is being made for you by a molecule. This creates a precarious dependency.
In the world of behavioural psychology, we examine the distinction between a “state” and a “trait.” The drug changes your state (you feel less hungry), but it does not change your traits (your habits, your coping mechanisms, your identity). If the individual doesn’t use the quiet period provided by the medication to do the hard work of identity change—learning to cook, finding joy in movement, managing stress without sugar—they are merely “renting” their new weight.
The “war” mentioned in the source involves more than just stomach growls. It involves your relationship with your environment. We live in an “obesogenic” environment that triggers our reward centres at every turn. Biological suppression addresses the signal of hunger, but it does not address the reasons for the consumption. If your eating is a response to a lack of purpose or chronic cortisol elevation, removing the physical sensation of hunger will only lead to the “boredom” of the drug. You will eventually find other ways to self-soothe, or the old patterns will come roaring back the moment the medication is withdrawn and the “noise” returns at double the volume.
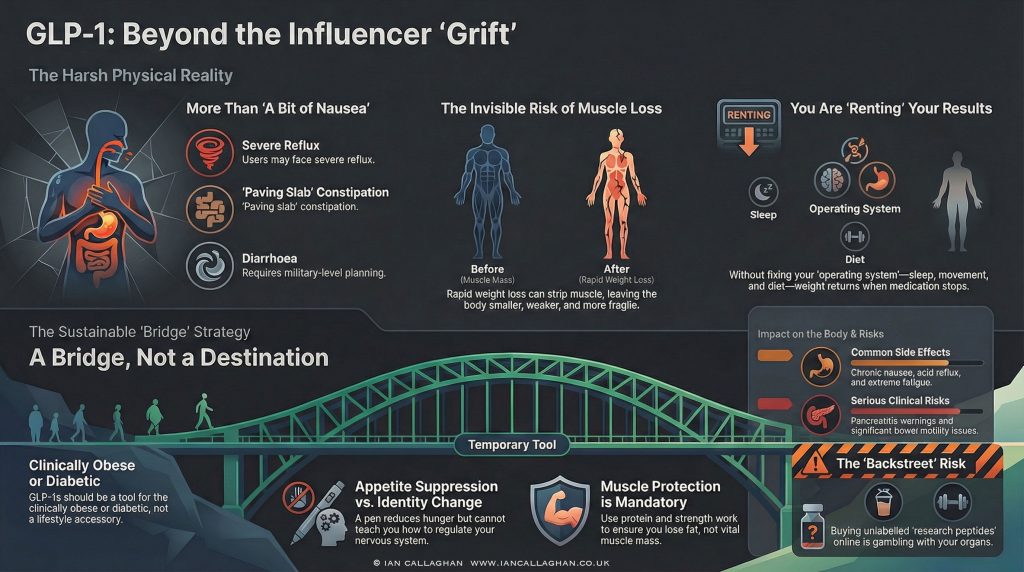
5. The Brutal Physical Toll: Beyond “A Bit of Nausea”
One of the most dangerous aspects of the GLP-1 graft is the deliberate minimisation of side effects. Influencers and predatory online clinics often dismiss the physical toll with breezy phrases like “a bit of nausea” or “minor digestive upset.” The reality for many users is far more brutal and decidedly less social media-friendly.
Data from the MHRA’s Yellow Card scheme in the UK has seen a surge in reports of adverse reactions as prescriptions have risen. These are not “cute little quirks”; they are significant physiological disruptions that can derail a person’s life. The reality of these effects includes:
- Persistent, Grinding Nausea: Not a fleeting feeling, but a sensation that hangs around from the moment you wake until you go to sleep, making the thought of even healthy food repulsive.
- Violent Vomiting: Frequent and unpredictable bouts of sickness that can lead to dehydration and electrolyte imbalances.
- Severe, Burning Reflux: Acid reflux so intense it can cause sleep deprivation and damage the oesophageal lining.
- “Paving Slab” Constipation: A sensation of extreme heaviness where the bowels simply stop moving. This is not just uncomfortable; it can lead to faecal impaction and require medical intervention.
- Military-Style Toilet Mapping: Conversely, some suffer from sudden, explosive diarrhoea that requires them to map out every public restroom on their commute like a tactical operation.
- Crushing Fatigue: A level of exhaustion that feels like the flu, wiping out the ability to work, socialise, or engage in the very exercise needed to protect muscle mass.
- Total Food Aversions: A loss of the “hedonic” pleasure of eating, where consuming any food becomes a chore that induces disgust.
Beyond these common experiences, there are serious, documented medical risks. The MHRA and the FDA have issued warnings regarding pancreatitis—a life-threatening inflammation of the pancreas—and bowel motility issues (gastroparesis), where the stomach effectively becomes paralysed. To frame these drugs as a “lifestyle accessory” for someone who just wants to lose half a stone for a wedding is a dangerous dereliction of duty.
“If someone’s selling this like it’s a lifestyle accessory, they’re a liar or an idiot. Sometimes both.”
When you choose a GLP-1, you are making a medical trade-off. You are potentially exchanging the burden of obesity for the burden of significant physical illness. For those at high clinical risk, this trade is often worth it. For the “biohacker” or the influencer looking for a shortcut, it is a reckless gamble.
6. The Quiet Disaster: The High Cost of Muscle Loss
While the scale might show a lower number, a “quiet disaster” is occurring beneath the surface for many GLP-1 users: rapid loss of lean muscle mass. This is the physiological trap that many influencers fail to mention because they are obsessed with “weight” rather than “composition.”
When weight loss is too rapid—often the case with GLP-1s due to extreme calorie deficits—the body does not just burn adipose tissue (fat). It looks for easier fuel, often stripping away the very muscle that keeps our metabolism functioning. This leads to a condition known as sarcopenic obesity. In this state, an individual may appear “thin” in clothes, but their body fat percentage remains dangerously high because their muscle mass has cratered. They become “smaller and more fragile,” rather than healthy.
Statistically, the data is alarming. In clinical trials such as the STEP 1 trial for semaglutide, body-composition substudies indicated that a significant portion of the weight loss—up to 40% in some cohorts—was lean mass. In the UK, where we already face an ageing population and rising rates of frailty, the move toward mass-prescribing these drugs without a mandatory emphasis on high protein intake and resistance training is a public health time bomb.
Muscle is your metabolic currency. It regulates your blood sugar, supports your skeletal structure, and helps prevent your basal metabolic rate (BMR) from plummeting. Protecting muscle is a “future-dependent” necessity. If you lose 4 stone but can no longer lift your groceries or walk up a flight of stairs without trembling, you haven’t improved your health; you have traded one form of metabolic dysfunction for a more fragile version. As the source context warns: “That is not health.” You must protect your muscles like your life depends on it, because it does.
7. The Alcohol Misconception: Solving the Wrong Problem
A trending narrative suggests that GLP-1s are a “cure” for alcohol addiction because some users report a decreased desire to drink. While the science of how these drugs interact with the brain’s reward centres (the mesolimbic pathway) is fascinating, the idea that a pen can “fix” alcoholism is a dangerous misconception that fundamentally misunderstands the nature of addiction.
Alcohol addiction is not an “appetite” problem. It is a “nervous system regulation” problem. People do not drink to excess because they have a “hunger” for the taste of gin in the same way they might want a sandwich. They drink to “change state”—to switch off the screaming noise of stress, loneliness, overwhelm, or trauma.
While a GLP-1 might temporarily dampen the impulsive “hit” of a drink, it does not touch the core problem of emotional dysregulation. If you are using a chemical “off switch” to handle your life, you haven’t fixed the life. You’ve just changed the switch. The “work” of sobriety and mental health is the “rebuild”—learning how to sit in the visceral discomfort of a bad day without reaching for a substance to numb your nervous system.
Using a GLP-1 as a crutch for alcohol issues without intensive therapy and lifestyle restructuring is just another form of “renting” a solution. It doesn’t teach you how to regulate your emotions. When the drug is stopped, the underlying trauma or stress-response is still there, waiting. Real recovery is about building a life you don’t need to escape from with chemicals.
8. The Backstreet Biohack: Gambling with Organs
The most alarming trend in the “GLP-1 Grift” is the rise of the “backstreet” or “grey market” version of these drugs. Desperate to bypass the high costs of private prescriptions (often £200-£400 per month) or the endless NHS waitlists, people are turning to “research peptides” and unlabelled vials sourced from questionable websites.
This is not “biohacking.” This is gambling with your organs in a game where the house always wins. When you purchase mystery semaglutide from an unregulated source, you are bypassing every safety protocol that exists in modern medicine. The risks are profound:
- Contamination: These vials are often produced in labs with zero oversight. They can be contaminated with heavy metals, dangerous bacteria, or unlisted fillers.
- Cold-Chain Failure: GLP-1s are proteins that require strict refrigeration. Grey-market shipping often disregards “cold-chain” integrity, meaning the substance can degrade into something toxic or simply inert by the time it reaches your door.
- Bacteriostatic Water Contamination: Many users are “reconstituting” powders themselves using unsterile water, leading to a high risk of abscesses and systemic infection.
- Wild Dosing Inaccuracy: An investigative look at these sources found concentrations to be wildly different from the labels. You could be injecting ten times the intended dose, leading to acute pancreatitis or severe hypoglycaemia.
Sourcing dosing advice from a TikTok comment section rather than a clinical professional is a recipe for a medical emergency. These are powerful hormones that affect the pancreas, the liver, and the brain. To treat them like a “backstreet” lifestyle hack is a level of risk that no aesthetic goal can justify. You only have one liver; don’t trade it for a cheaper dress size.
9. Renting Results: The ‘Bridge’ vs The ‘Destination’
So, what is the “Sane Position” on GLP-1s? They are a tool, and for the right person, they can be a “useful bridge.” That person is typically someone who is clinically obese, diabetic, facing high cardiovascular risk, or trapped in a binge-eating cycle that makes traditional lifestyle changes feel impossible. For them, the drug can lower the “noise” enough to allow them to cross the bridge from chronic illness toward health.
The problem arises when the drug is treated as the “destination.” If you use the pen to lose weight while maintaining a life of “chaos,” you are merely renting your results. In the UK, “chaos” is often synonymous with our food environment. We have the highest consumption of Ultra-Processed Foods (UPFs) in Europe, with UPFs making up over 50% of the national diet. As DDrChris van Tulleken has documented, these foods are designed to bypass our satiety signals.
Living in chaos looks like:
- Continuing to rely on UPFs and “diet” rubbish while on the drug.
- Drinking heavily every weekend, relying on the drug to “cancel out” the calories.
- Refusing to address sleep hygiene (which regulates ghrelin and leptin).
- Ignoring chronic stress and the “cortisol belly.”
- Remaining sedentary while the drug strips your muscles.
When you stop taking the drug—and for most, the “rental agreement” will eventually end due to cost, supply issues, or side effects—the “old operating system boots back up.” Your body’s biological “set point” will fight to return to its previous weight. If you haven’t used the “quiet” provided by the drug to rebuild your habits and repair your metabolism, your biology will revert, often with a “rebound” effect where ghrelin levels (the hunger hormone) skyrocket and leptin sensitivity (the fullness signal) remains low. You cannot medicate your way out of a lifestyle that is fundamentally broken.
10. Conclusion: Rebuilding the Operating System
The GLP-1 era has brought a powerful medical tool into the spotlight, but it has also empowered a new generation of grifters who value profit over patients. These drugs represent a significant advancement in metabolic science, capable of quietening the biological “war” of hunger that plagues so many. However, we must stop pretending they are a substitute for the “messy, earned” work of rebuilding a life.
A GLP-1 can reduce your appetite, but it cannot repair your relationship with yourself. It cannot teach you how to handle the “3 am ceiling stare” without a “chemical off switch.” It cannot build the muscle that will protect your independence as you age. And it certainly cannot provide the identity shift required to maintain health in an environment designed to make you sick.
If you are considering these tools, or already using them, you must ask yourself a difficult, honest question: Are you looking for a temporary rental, or are you ready for a permanent architectural change in your health?
If you use the drug to mask the chaos of a poor diet, lack of movement, and unmanaged stress, you are simply delaying the inevitable. The “old operating system” is always waiting to boot back up, and it is a relentless programmer. The real “miracle” isn’t found in a pen; it is found in the boring consistency of real food, the fierce protection of your physical strength, and the courage to stop negotiating with your self-destruction.
GLP-1s can lower the volume of the noise, but you are still the one who has to decide what to do with the silence. Make sure you are building something that lasts long after the prescription runs out.
The 30-Day Reset: Reclaim Your Vitality, Rewire Your Mind, and Reboot Your Body (Digital Ebook)
Stop feeling like a deflated balloon stuffed with sawdust. If you are ready to fix gut health over 40 and finally end the cycle of brain fog and “gut rot,” you need a tactical reboot. My name is Ian Callaghan—Chef, Nutritionist, and former Soldier. I’ve lived the contradiction of professional kitchens and military trenches, and I know exactly why you’re wired, tired, and fed up.
Great breakdown of how GLP-1 treatments are reshaping the weight-loss landscape it’s crucial to stay aware of both medical benefits and market tensions.
For a deeper look at the competitive and legal dynamics around GLP-1 pricing and brand protection, this link offers useful insight: https://wegovypricecompare.com/glp-1-drug-wars-wegovys-maker-targets-knock-off-competitors/