Why Your Mental Health Is a Hardware Failure
A Veteran’s Guide to Metabolic Sovereignty
Introduction: The 3 AM Siege
It is 03:00, and you are staring at the ceiling while your body behaves as if the room has been breached. Your heart is hammering against your ribs, your skin is clammy, your mouth is dry, and your breathing has gone shallow in that horrible way that makes the air itself feel thick. Your mind is nowhere near your bedroom. It is out on exercise somewhere, or back in a place you thought you had left behind years ago, or trapped in a full-scale internal assault made up of dread, regret, shame, unfinished business, future fear, and every other bastard thought that likes to show up when the world is dark and quiet enough for your nervous system to start making threats out of static.
In the civilian world, they have names for this. They call it anxiety. They call it panic. They call it generalised anxiety disorder. They call it a mental health crisis. Then they sit you in a chair, ask you how you felt about your childhood, and hand you a label as if naming the fire is the same thing as putting it out. Then, if that does not work, they medicate the signal without asking what the signal is actually trying to tell you.
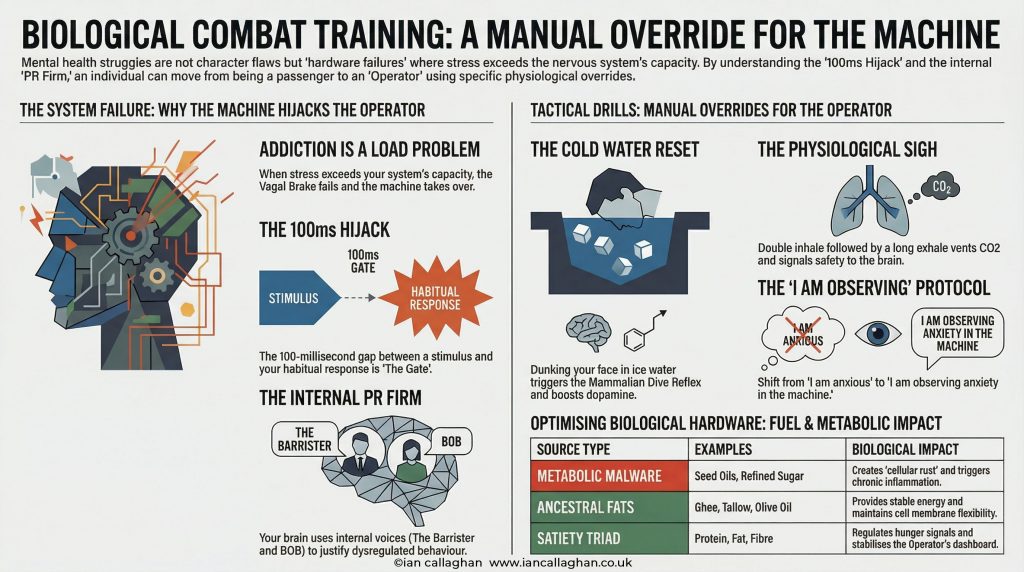
I call it a hardware failure.
That does not mean life experience is irrelevant. It does not mean trauma does not matter, grief does not matter, military service does not matter, money pressure does not matter, loss does not matter, sleep deprivation does not matter, and the accumulated weight of a hard life does not matter. Of course it bloody matters. But if the hardware underneath all of that is failing, you are not dealing with a purely psychological event. You are trying to fight a war with a jammed weapon while people around you keep insisting the problem is your attitude.
That is where so many people get completely shafted. They are told their suffering is a mindset problem, a personality problem, a weakness problem, a story problem, when in reality their internal machinery is running on industrial sludge, broken signalling, chronic inflammation, unstable blood sugar, poor sleep, dehydration, low minerals, a compromised gut, and a nervous system that has forgotten where the off switch is. You can talk all you like in that condition. You can journal about it, analyse it, intellectualise it, and build a beautifully articulated explanation for why you feel the way you feel. But insight does not repair biology. A body that is physically redlining does not give a shit how self-aware you are.
I speak from the perspective of an Operator. During my time in the British Army, I learned very quickly that a Forward Operating Base is only as secure as its perimeter and its supply lines. If the perimeter is breached, everything inside becomes unstable. If the fuel is contaminated, vehicles fail. If the comms go down, bad decisions multiply. If the supply chain is corrupted, the mission degrades no matter how disciplined the men are. It does not matter how good the operator is if the hardware is compromised. It does not matter how brave the pilot is if the engine is seizing up. And it does not matter how much positive thinking you throw at a body that is inflamed, undernourished, overclocked, poorly slept, and drowning in modern metabolic sabotage.
I spent forty years in the world of food and nutrition. I have lived through the terrain of PTSD. I lost 5 stone of protective armour I had built around myself, dragged myself back from the brink of pre-diabetes, and built fifteen months of hard-won sobriety not through hollow willpower theatre, not through pretending cravings did not exist, and not through surrendering my agency to some external doctrine, but through engineering. That is not a motivational line. That is lived experience. It matters because most people have been sold the wrong story about what is happening to them.
They have been told that if they are anxious, flat, reactive, exhausted, overwhelmed, panicky, volatile, depressed, or full of dread, then something in them is morally wrong, psychologically defective, or permanently broken. No. Sometimes what is wrong is not your soul. It is your fuel, your signalling, your gut, your inflammatory load, your sleep architecture, your blood sugar volatility, and your nervous system trying to survive inside a biological environment that keeps screaming danger. The problem you are facing at 03:00 is not necessarily a character flaw. It is not proof that you are weak, broken, or naturally doomed to darkness. It may be proof that your internal hardware is under siege.
And while that siege continues, another bastard always comes online.
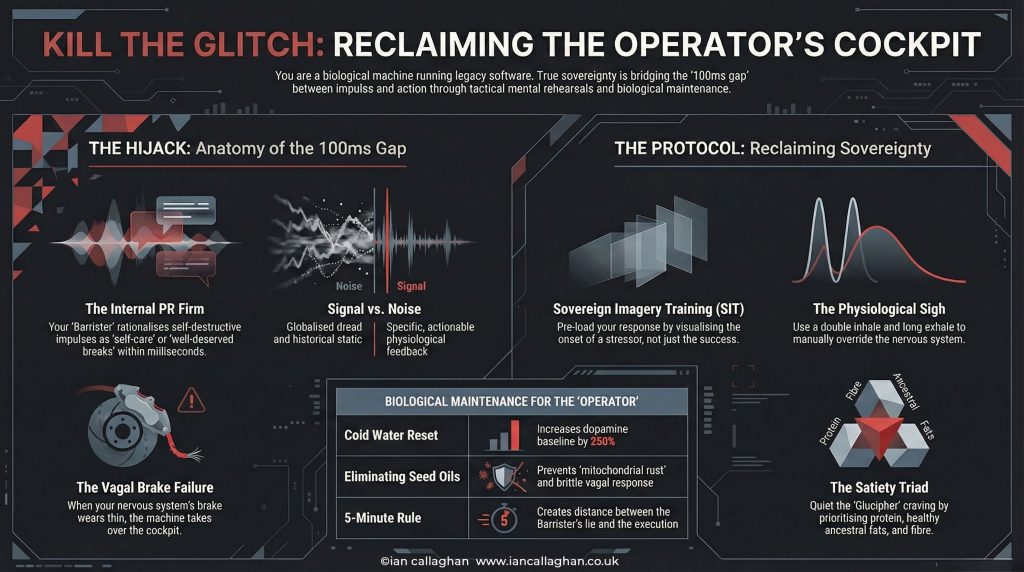
I call him the Internal Barrister.
That relentless voice in your head has spent years building a case against you. It rifles through your past like a prosecution file and presents your failures, relapses, panic episodes, binges, shutdowns, overreactions, bad calls, old wounds, and worst moments as evidence that you are fundamentally defective. It does not defend you. It indicts you. And because the machine underneath is throwing danger signals all day long, the Barrister sounds convincing.
Mission Log: The Hyper-Vigilance Loop
I remember being on night patrol with every sense dialled right up. In that environment, hyper-vigilance is not an illness, it is an advantage. It keeps you alive. Every sound matters. Every movement matters. Every subtle shift in atmosphere matters. The problem starts when you come back into civilian life and the body does not get the memo. The same state that once protected you begins turning on you. You walk into a supermarket and your heart redlines. A sound behind you makes your body jolt before your mind has caught up. You wake at 03:00 like a man under attack and start believing you are mentally ill.
That was the lie I believed for years. I thought my mind was broken. I thought I was defective. I thought I had simply become one of those people who could no longer cope. What I eventually realised was much uglier, much less fashionable, and much more useful. My FOB was under siege from the inside. My hardware was malfunctioning. My internal systems were drowning in inflammation, unstable fuel signals, poor recovery, and biological noise. My brain was not inventing danger out of nowhere. It was receiving danger signals from inside the perimeter.
This guide is a tactical manual for reclaiming metabolic sovereignty. We are going to stop treating you like a passive component in a broken system, stop pretending labels are solutions, and stop worshipping analysis while ignoring chemistry. Then we are going to start treating you like the Operator in the cockpit, because when the machine works better, the software stops screaming quite so loudly.
The Gut as the Operating System: Beyond the Mental Health Story
If a radio signal is garbled, you do not start by blaming the operator. You check the antenna, the battery, the wiring, and whether something is jamming the signal. That is basic field logic. Yet when people feel anxious, flat, panicked, unstable, reactive, or like they are one bad conversation away from coming apart, the modern system makes it a story about personality almost immediately. You are too sensitive. You are stressed. You are wired this way. You are overthinking. You are mentally unwell. You need coping strategies.
Maybe. But maybe your operating system is compromised.
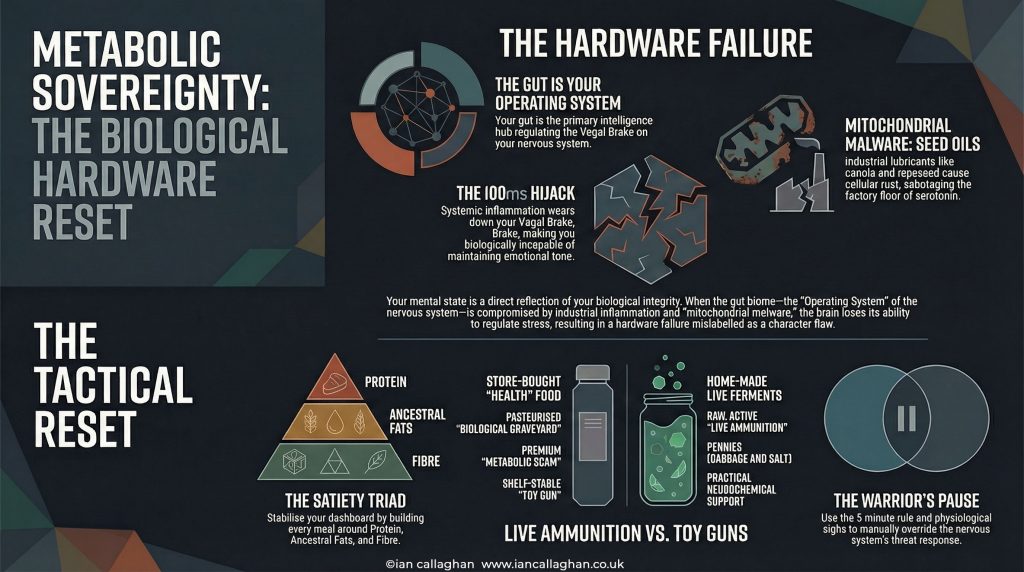
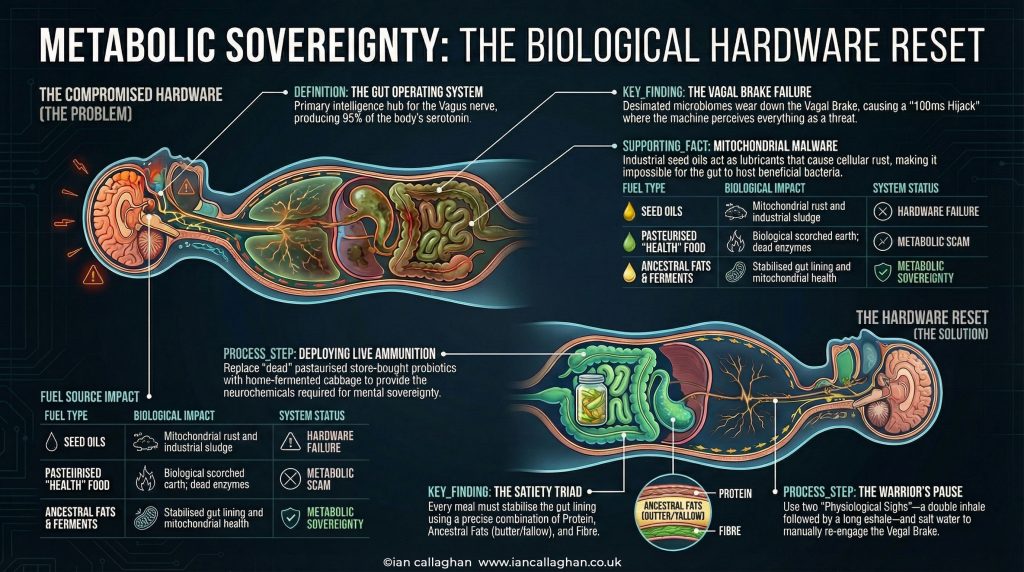
Your gut is not just a digestive chute. It is not a passive sack where calories get dumped and sorted while the grown-up systems get on with the important work. It is one of the major intelligence hubs of your nervous system, deeply involved in signalling, regulation, immune activity, inflammation, and the constant conversation between brain and body. When that system is inflamed, damaged, underfed, overprocessed, chemically irritated, or biologically starved, the signal-to-noise ratio across the whole machine changes. You do not just feel a bit off. You become harder to regulate, harder to settle, harder to reassure, harder to stabilise, harder to sleep, harder to motivate, harder to soothe, and harder to trust. That is not weakness. That is corrupted signalling.
The Path of the Vagus Nerve
At the centre of this sits the vagus nerve, one of the major communication lines between brain and body. It runs from the brainstem down through the neck, into the chest and abdomen, linking the brain with the heart, lungs, digestive tract, and other systems that have an awful lot to do with whether you feel safe or under threat. I think of it as both the comms wire and the brake line, because one of its main roles is helping regulate the shift between threat mode and recovery mode, between fight or flight and rest, digest, recover, and repair. That is what I mean when I talk about the vagal brake.
When that brake is in decent condition, life can still hit hard without knocking you clean out of the cockpit. You can receive bad news, stress, criticism, setbacks, and uncertainty without instantly tipping into panic, fury, or collapse. Not perfect calm, not monk mode, just enough space between stimulus and reaction that you remain involved in your own response. But when the system underneath is inflamed, exhausted, over-caffeinated, undernourished, poorly slept, gut-wrecked, and constantly pushed, the brake wears thin. Then everything gets louder, faster, more personal, and more threatening. People start saying they do not feel like themselves, cannot cope with simple things, keep snapping, cannot calm down, feel wired and tired, and cannot switch their mind off. That is not always a personality problem. Sometimes it is faulty hardware screaming through damaged comms.
The 100ms Hijack
That leads to what I call the 100ms Hijack. In a more regulated state, there is a tiny gap between something happening and your reaction to it. A noise, a message, a memory, a stressor, a craving, a criticism, a look, a comment, a trigger. That tiny gap is where sovereignty lives. It is where you can notice a thought without obeying it, feel a craving without becoming it, hear the Barrister without hiring him, and experience a spike of emotion without handing over the keys.
But when the hardware is failing, that gap all but disappears. You go from stimulus to reaction with nothing useful in between. A look becomes a threat. A craving becomes an instruction. A thought becomes a command. A sensation becomes a catastrophe. That is the hijack, and it is the bit most people miss. You are not just unhappy. You are not just overthinking. In that moment, you may be biologically incapable of maintaining enough regulation to stay in command. Which is exactly why being told to just calm down is so useless. Calm is not a moral achievement. It is often the downstream result of a system that is not overloaded.
You have listened to the Internal Barrister for so long that you have started accepting its case notes as autobiography. You are wrong. You do not necessarily have a character flaw. You may have a hardware failure.
Stop Talking, Start Fixing
The modern wellness world loves a post-mortem. It loves digging around in your past, naming your wounds, categorising your trauma, and building an endless museum of explanation. Some of that has its place. Understanding matters. Context matters. Language matters. But understanding does not automatically alter state. You can have perfect insight into why you felt abandoned at seven years old and still wake up at 03:00 with your heart trying to punch through your ribs because your gut is inflamed, your blood sugar has crashed, your sleep is broken, your nervous system is fried, and your chemistry is screaming danger.
That is why I keep coming back to the same brutal point. You are trying to debug software on a machine with a damaged motherboard. Stop talking. Stop over-analysing. Stop mistaking awareness for repair. Start fixing the hardware.
The Metabolic Scam: Why Your Health Food Is a Graveyard
The modern supermarket is a minefield disguised as convenience, and most of what is sold as healthy is not there to restore you. It is there to monetise confusion. That is where another bastard enters the frame.
Glucipher.
Glucipher is my name for the metabolic scam artist built into the modern food environment. He is the smiling salesman behind the healthy aisle, the one who takes industrial rubbish, wraps it in soft language, sticks earthy colours on the label, adds words like natural, organic, probiotic, gut-friendly, plant-based, functional, balanced, and alive, and then charges you a premium for something that often has all the life force of a brick. He loves your confusion, feeds on your lack of sovereignty, and wants you trapped between obvious junk food and fake health food forever, because a confused customer is a profitable customer.
Biological Scorched Earth
Take supermarket sauerkraut or kombucha. People buy this stuff thinking they are doing something deeply therapeutic for their gut. Sometimes they are, but a lot of the time they are buying an expensive story in a jar. To make fermented products shelf-stable for months on end, many manufacturers pasteurise them. In plain English, they heat the thing until they kill the very bacteria and enzymes that made it useful in the first place. That is biological scorched earth. They kill the live activity, flatten the culture, and make it warehouse-safe, transport-safe, and shelf-safe. Great for logistics. Shit for biology.
Then, because people have wrecked their taste buds on sugar and ultra-processed sludge, the same industry often sweetens the product or engineers it to fit the civilian palate. So now you are not even paying for living support. You are paying for a sanitised corpse in lifestyle packaging. You are not buying medicine. You are buying a graveyard.
Live Ammunition vs Toy Guns
This is the part that should properly piss people off, because you can make live fermented food on your own kitchen counter for pennies. A cabbage, some salt, a jar, and a bit of patience. That is it. No influencer starter kit, no shiny subscription, no gut protocol PDF written by someone with ring lights and no field scars, and no £8.50 wellness theatre in a recycled glass bottle. Just real biological activity.
That matters because sovereignty begins when you stop outsourcing repair to corporations that make money from your maintenance, not your recovery. Why would you trust the same machine that filled the shelves with ultra-processed sludge to suddenly become your healer? Why would you hand your biology back to an industry that profits every time you stay confused, inflamed, bloated, undernourished, and emotionally unstable enough to keep buying fixes?
That jar of fermenting cabbage on your counter is not just food. It is a cheap, old-world, deeply unsexy act of self-governance. It is live ammunition. It is a basic neurochemical support system that bypasses the scam entirely.
Here is the difference in plain terms.
| Feature | Store-Bought Dead Version | Home-Made Live Version |
|---|---|---|
| Status | Often pasteurised and flattened | Raw, active, evolving |
| Content | Can include added sugar, preservatives, dead cultures | Cabbage, salt, water, bacteria doing their job |
| Potency | Decorative wellness | Practical biological support |
| Cost | £5 to £12 for branded nonsense | Pennies |
| Shelf life | Stable because it is sanitised | Alive because it is active |
That does not mean every shop-bought ferment is useless. Some are decent. Some are genuinely live. But most people do not even know to check, because they have been trained to buy the story instead of inspecting the hardware. That is how Glucipher works. He does not need to poison you outright. He just needs to keep you dependent.
Mitochondrial Malware: The Industrial Sabotage of Seed Oils
If your gut is part of the operating system, your mitochondria are the power plants. These tiny structures inside your cells produce actual cellular energy, the stuff that allows your body to run, repair, recover, regulate, and keep the lights on. And most people are uploading malware into those systems every single day.
I am talking about industrial seed oils. Canola, rapeseed, sunflower, soybean, corn oil, vegetable oil blends, and all the slippery beige bullshit hidden in dressings, sauces, snacks, ready meals, takeaways, protein bars, low-fat spreads, healthy wraps, fake food, and most of the rubbish people now call normal. Historically, these were not traditional foods. They were industrial oils later pushed deep into the food supply through mass processing, aggressive marketing, and the replacement of older, more stable fats with cheaper, more profitable modern substitutes.
That matters because these oils are not neutral passengers. When heavily consumed, especially in the context of ultra-processed modern diets, they increase oxidative stress, undermine stability, and add to the inflammatory burden that already overloaded bodies are struggling to carry. I call that cellular rust. And when you combine that rust with poor sleep, alcohol, chronic stress, blood sugar volatility, low protein intake, poor mineral intake, and a wrecked gut, the result is not just physical fatigue. It shows up as mental noise, poor resilience, lower stress tolerance, more cravings, more reactivity, and more internal static.
That does not mean one takeaway destroys your soul or one meal out poisons you forever. This is not about panicking over one portion of chips. It is about what happens when industrial oils become the default fuel line of your life.
The Enteric Nervous System: Your Second Brain
Your gut has its own nervous system, a huge network of neurons and signalling pathways that communicate constantly with the brain. Most of the body’s serotonin is produced in the gut, not the brain, which should wake people up to the fact that the terrain of the gut matters far beyond digestion. If that terrain is compromised, the downstream effects can show up as mood instability, poor sleep, altered appetite, anxiety, irritability, dread, and that weird flatness people often struggle to describe.
If the factory floor is flooded, production suffers. If the lining is inflamed, the microbiome is depleted, the incoming materials are industrial rubbish, and the whole system is running under chemical stress, then the production line for stability is compromised. The brain receives poor-quality information from below, and that is when another bastard takes the mic.
The PR Firm
The PR Firm is the part of your mind that creates polished excuses for broken biology. It tells you that you deserve a treat, that you have had a hard day, that it is just one drink, just one takeaway, just one little release, just one act of comfort, just one thing to take the edge off. It wraps self-sabotage in the language of self-care, which is one of the most dangerous tricks in the modern world. People end up dysregulated while believing that the very thing keeping them dysregulated is helping them cope. That is how the loop keeps going.
The Insulin Lock
This feeds into what I call the Insulin Lock. You can be carrying loads of stored energy on your frame and still feel constantly driven to eat, because access to energy and possession of energy are not the same thing. If your system is inflamed, over-insulinated, under-muscled, under-proteined, poorly slept, and metabolically inflexible, your body struggles to access what it has already stored. So the brain perceives emergency and starts screaming for quick fuel, sugar, bread, crisps, alcohol, pastries, anything that hits hard and fast.
Then the PR Firm steps in and builds a lovely little story about stress, comfort, reward, and deserving. But the underlying issue may be fuel access, inflammatory chemistry, and unstable signalling. You are not just weak. You are not just greedy. You are not just comfort eating because you lack discipline. You may be running a tanker with seized pumps.
That is a hardware problem.
Tactical Manual: The Satiety Triad for Metabolic Sovereignty
If you want to reclaim your biology, you need more than vague advice. You need an SOP, a repeatable operating procedure, a way of fuelling the machine that lowers noise, improves resilience, stabilises energy, and gives the nervous system half a chance of staying in command. I call this the Satiety Triad.
Every time you put something in the hole under your nose, it needs to earn its place. It needs to support the mission, not sabotage it. The three pillars are simple: protein, ancestral fats, and fibre. That is not trendy, sexy, or new, which is precisely why it works.
Protein: The Leverage Point
Protein is the anchor and the leverage point, the thing most people massively under-eat while wondering why they cannot stop thinking about food, sugar, or comfort. There is a biological principle often referred to as protein leverage. In practical terms, it means your body keeps pushing hunger signals until it gets enough of the building blocks it actually needs. If you keep feeding it low-protein, high-reward, high-energy, low-satiety rubbish, it does not calm down. It keeps asking, nudging, and driving appetite, and then people tell themselves they have no willpower.
No. They have unmet biology.
When you build meals around proper protein, the volume starts dropping. The scavenging drops. The sweet-tooth nonsense drops. The constant background hunt for dopamine through food starts easing. That is not magic. That is the machine finally getting what it has been asking for.
Ancestral Fats: Clean-Burning Fuel
You need stable fuel, not industrial lubricants dressed up as nutrition and not fake low-fat rubbish padded out with starches, gums, sugars, and marketing. I am talking about butter, tallow, egg yolks, quality dairy if you tolerate it, and extra virgin olive oil used properly. These foods are not just calories. They are structural. They support cell membranes, satiety, hormonal function, and calmer, steadier energy.
Ancestral fats are not a luxury. They are a return to fuels human biology actually recognises. When people are constantly hungry, emotionally volatile, and never satisfied, one of the first things I want to know is whether their meals are remotely built to satisfy a human nervous system. A low-fat yoghurt and a cereal bar is not a strategy. It is a setup.
Fibre: The Infrastructure
Not fibre powder in a shiny tub. Real fibre from real food, especially fibrous vegetables and fermented plant foods that actually give the gut something useful to work with. Cabbage, broccoli, kale, leeks, onions, garlic, and proper produce. This is the infrastructure, the scaffolding, the terrain support, the incoming material your internal ecosystem can actually use. Live fermented food brings the reinforcements. Fibrous whole food helps them hold the ground.
A Stable Mind Is Built on Stable Inputs
This is the bit most people miss. A stable mind is not built on slogans. It is built on stable inputs. If your blood sugar is bouncing all over the place, your gut is inflamed, your meals are beige processed convenience sludge, your nervous system is living on caffeine and cortisol, and you are under-eating protein while over-eating fake food, you will feel that. You will experience it as irritability, cravings, dread, poor sleep, low patience, intrusive food thoughts, overwhelm, and that sense that life is somehow louder than it should be. That is not all in your head. It is in your inputs.
Your First 24-Hour Loadout
If you want to reset the machine, start simple, not perfect. Breakfast can be three eggs cooked in butter or tallow, with no toast, no orange juice, and no cereal pretending to be breakfast, plus some live fermented cabbage on the side if you have it. The tactical purpose is obvious: protein early, stable fats early, and no sugar bomb to send you crashing mid-morning.
Lunch can be steak, mince, chicken, sardines, salmon, or whatever proper protein you can actually afford, with a massive side of green veg and some extra virgin olive oil or butter where appropriate. That is about maintaining tone, reducing snack drive, and avoiding the post-lunch sedation that follows high-carb, low-protein nonsense.
Dinner can be fish, lamb, beef, eggs, or another solid protein source, backed up by more fibrous veg and more live fermented support. The job there is to provide repair materials, steadier overnight chemistry, better satiety, and a better chance of sleeping without your body behaving as if it has been abandoned.
And yes, throw the rapeseed oil in the bin. It belongs in machinery, not in your mitochondria.
The Warrior’s Pause: Implementing the 5-Minute Rule
Even when you improve the hardware, you are still dealing with legacy software, old loops, cravings, patterning, escape routes, and reward maps. That is why people get confused. They clean up their food for a week, feel a bit better, then a craving or stress response hits and they conclude that nothing has changed. No. Something has changed. You are just still carrying old code, which is where you need a manual override.
I call it the Warrior’s Pause.
The 5-Minute Rule
When the noise starts, do not negotiate with it, philosophise about it, or let the PR Firm narrate it into something meaningful. Do not let the Internal Barrister turn it into proof that you are fucked. Run the drill. First, stop and recognise that the thought, craving, urge, or panic spike is a signal, not a command. You do not need to obey every signal your body throws.
Then use the physiological sigh. Inhale through the nose, take a second, smaller inhale at the top, then exhale slowly through the mouth until the lungs empty. Do it a few times. It is not magic. It is mechanics. You are using breath to influence state and giving the brake line a chance to engage.
Then hydrate properly. A lot of what people read as hunger or anxiety is dehydration, stress chemistry, mineral depletion, or simple physiological noise. Drink water, and use a pinch of decent salt if appropriate for you. Then wait. Give the system five minutes, not to become enlightened, but to lose some of the hijack.
Mission Log: The Sobriety Fight
During early sobriety, the Internal Barrister was loud. Very loud. It would tell me I had earned a drink, needed a drink, could not handle the symptoms without a drink, and that one drink would shut the noise down. I did not beat that by arguing with it for an hour. I beat it by learning not to treat every urge like truth.
Water. Salt. Breath. Pause. Protein. Walk. Reset.
That was the difference. I stopped debating the craving and started servicing the machine, which is a very different war.
Reclaiming the Gate: Firing the PR Firm and the Internal Barrister
The gate is that narrow point between signal and action, the space where choice either survives or disappears. When the hardware is wrecked, the gate gets overrun. When the hardware is better supported, the gate gets stronger. That matters because if there is no gate, there is no sovereignty.
Firing the PR Firm
The PR Firm is smooth, articulate, emotional, and persuasive. It takes self-sabotage and wraps it in comforting language. You deserve this. You need this. You have had a long day. This is self-care. Do not be extreme. One will not matter. Life is short. It sounds compassionate, but often it is treachery, because it is not speaking for the Operator. It is speaking for the pattern, the urge, Glucipher, and the part of the machine that wants immediate relief even when that relief deepens the long-term problem.
You need to stop treating that voice as wisdom. It is not wisdom. It is public relations for bad decisions.
Silencing the Internal Barrister
The Internal Barrister is more brutal. It is not soothing, it is prosecuting. It digs up old evidence, the panic attack in Tesco, the binge, the relapse, the cancelled plan, the mood swing, the period when you could barely function, the days you hid, the years you numbed, and then it stands in the court of your mind and says, see, this is who you are: weak, broken, unstable, hopeless, beyond repair.
But the Barrister is only as good as its data, and when your biology is screaming danger all the time, the data is corrupted. It mistakes symptoms for identity, state for character, and overload for truth. You do not have to kill it with some magical affirmation. You just have to stop letting it pass bad data off as final verdict.
Operator vs Component
A component is moved by external forces. Sugar pulls it, alcohol pulls it, seed oils pull it, poor sleep pulls it, stress chemistry pulls it, old urges pull it, social pressure pulls it, and metabolic noise pulls it. A component reacts, obeys, and gets dragged.
An Operator observes, assesses, adjusts, and responds. An Operator does not worship every impulse.
You are not your thoughts, cravings, panic spike, the Barrister, or the PR Firm. But you will struggle to observe any of that clearly if the lens is covered in the soot of a failing biome. This is not wellness. Wellness is a soft, polished word for people who have never had to fight for their own mind. This is metabolic sovereignty, and it is not about perfection. It is about reclaiming enough internal order that you are no longer permanently operated by noise.
The Mechanic’s Mindset: Data Over Verdicts
When a Land Rover breaks down in the middle of nowhere, the mechanic does not sit on the floor beside it wondering whether the engine feels supported. He checks the fuel, the battery, the lines, and what failed. No melodrama, no identity crisis, and no moral judgement. Just diagnosis.
That is the mindset you need, because one of the main reasons people stay stuck is that they treat every bad day as a verdict on who they are. Bad sleep becomes, I am broken. A panic spike becomes, I will always be like this. A craving becomes, I have failed. A mood dip becomes, something is wrong with me.
No. It is data.
Not all of it, not always, but far more of it than people have been taught. So when the check engine light comes on, stop turning it into theology. Run the checks. Tone check. How fried am I right now? Fuel check. What have I actually eaten, and did I feed the machine or wind it up? Sleep check. Did I recover or just sedate and collapse? Gut check. Have I done anything this week that actually supports the operating system? Stress load check. Am I carrying something real here, or pretending biology and life are separate when they are colliding in real time?
When I lost 5 stone and dragged myself back from pre-diabetes, I did not do it by finding myself, saying nicer things in the mirror, or becoming spiritually superior. I did it by treating my body like high-performance hardware that had been run badly for too long. I cleaned the fuel lines, changed the inputs, stopped feeding the sabotage, and started respecting biology. The noise changed. Not overnight and not perfectly, but measurably, reliably, and deeply.
That matters because once you realise some of your suffering is mechanical, the whole conversation changes. Now you are not a broken person waiting to be saved. Now you are an operator learning how to service the machine.
Conclusion: Reset the Clock
The reset clock is always running. It does not care about good intentions, saved posts, motivational screenshots, podcasts, or your plan to start on Monday. It responds to inputs, patterns, repetition, and the daily servicing of the machine.
Every day you choose stable fuel over industrial rubbish, you lower noise. Every day you choose protein over beige convenience nonsense, you improve leverage. Every day you choose live food over dead packaged theatre, you support the operating system. Every day you choose pause over impulse, you strengthen the gate. Every day you choose to act like the Operator instead of the component, you reclaim a bit more sovereignty.
That is how the brake strengthens, how the 100ms gap widens, how the Internal Barrister loses its case, how the PR Firm gets fired, and how you stop confusing broken signalling with broken identity. Your mental health is not always a mystery. Sometimes it is a message from the hardware.
Not all of it. Not every part. Not every case. But far more than people have been taught.
You cannot think your way out of a hardware failure. You have to work your way out of it, one meal, one breath, one pause, one choice, one reset at a time.
The Warrior’s Command
Get the cabbage. Buy a head of cabbage and some proper salt, then start the ferment. Build your own neurochemical support instead of funding the scam.
Get the jar. Stop waiting for ideal conditions and start where you are. The factory does not build itself.
Kill the malware. Purge the seed oils and fake health rubbish from your kitchen. Stop uploading sabotage into your own power plants.
Reclaim the gate. When the noise hits, use the physiological sigh, hydrate, pause, and step back into the cockpit.
Track the machine. Stop treating symptoms as identity and start reading them as signals.
Operate.
Because the truth is brutal, but freeing. A lot of what you have been calling a broken mind may actually be a body under siege. A lot of what you have been calling weakness may actually be bad inputs, corrupted signalling, low resilience, and mechanical overload. A lot of what you have been calling you may actually be noise.
So the real question is this. Is your lens clear enough to see the Operator, or are you still blinded by the soot of a failing biome?
The briefing is over. The mission is clear.
Stand up. Reset the clock. Operate.
FAQ: The Questions People Usually Ask Once They Stop Calling It a Character Flaw
Can gut health really affect anxiety and panic?
Yes, it can, and not in a fluffy magazine way, in a very real signalling way. Your gut is connected to your nervous system through multiple pathways, including the vagus nerve, immune signalling, hormonal responses, and the production of key compounds involved in mood and regulation. If the gut environment is inflamed, depleted, or constantly irritated, that can feed into how you feel mentally and emotionally. It does not mean every panic attack starts in the gut, but pretending the gut has nothing to do with anxiety is outdated rubbish.
What is the vagus nerve and why does it matter so much?
Think of the vagus nerve as one of the major lines of communication between your brain and body. It helps regulate heart rate, digestion, stress responses, and the shift between fight-or-flight mode and recovery mode. When people talk about being stuck in overdrive, the vagal system is often part of the conversation. A healthier, better-supported system generally has more braking power. A wrecked, overloaded system tends to redline more easily.
Are seed oils really that big a problem?
The issue is not that one mouthful of sunflower oil turns you into roadkill. The issue is chronic load. These oils are everywhere in the modern food environment, especially in ultra-processed food, takeaways, sauces, snacks, and ready meals. When that becomes the default pattern, it adds to oxidative stress, inflammation, and metabolic dysfunction. The problem is not one exposure. The problem is the background load created by constant exposure.
Why does protein help with mood and cravings?
Protein is not just for muscles. It supports satiety, neurotransmitter production, tissue repair, and blood sugar stability. When people massively under-eat protein, they often get dragged around by appetite, low resilience, and constant food noise, then blame themselves for it. Better protein intake does not solve every emotional problem on earth, but it often lowers the volume of chaos in ways people notice quickly.
Is this saying trauma and life stress do not matter?
No, that would be stupid. Trauma matters. Loss matters. Relationships matter. Money stress matters. Military experience matters. Grief matters. Life matters. The point is not that biology is the only layer. The point is that biology is a massive layer that gets ignored while people are encouraged to analyse themselves on top of broken hardware. Both can matter, but if the body is under siege, the mind will feel it.
Can changing food really make that much difference?
For some people it makes a dramatic difference. For others it is one major piece of a bigger puzzle. But either way, better food, better protein, better fats, fewer industrial inputs, more live food, and more stable blood sugar usually give the nervous system a better environment to function in. You do not need to worship food. You just need to stop pretending it has no effect on the machine.
Why call it metabolic sovereignty?
Because sovereignty means self-governance. It means reclaiming authority over your own internal territory instead of living as a managed component in someone else’s industrial system. Metabolic sovereignty is about taking back control of the inputs, rhythms, and behaviours that shape your energy, mood, cravings, resilience, recovery, and capacity to operate. It is the opposite of outsourcing your biology to a machine that profits from your confusion.
What is the first thing I should actually do?
Do not start with twenty rules and a panic attack. Start simple. Get proper protein into your meals. Remove the obvious industrial rubbish. Hydrate properly. Get some daylight. Use the physiological sigh when the system redlines. Make one jar of live fermented cabbage. Build from there. You do not need a perfect protocol. You need a first act of sovereignty.

Metabolic Sovereignty: Silence Food Noise & Fix Your Metabolism
Tired of the “Food Noise” and the afternoon energy crash?
Under Load by Ian Callaghan | The Mechanical Guide to Addiction Recovery
You already know what you’re doing. You’ve known for years.