Emotional Sobriety: What Nobody Tells You About Being Sober But Still a Mess
Emotional Sobriety. You stopped drinking. So why are you still losing your shit?
You did the hard part. You put the drink down. Maybe you white-knuckled it; maybe it clicked one day, and you just stopped; maybe you did it quietly without telling anyone. Either way, you did it.
And then you waited for the life you were promised.
The calm. The clarity. The version of yourself you always knew was in there somewhere, buried under the years of numbing. You waited for the relationships to heal, for the decisions to get easier, for the anger to lift. You waited to feel like a functioning human being who wasn’t one bad moment away from saying something they couldn’t take back.
But the anger didn’t lift. The reactivity didn’t go. You’re still snapping at people who don’t deserve it—still lying awake replaying conversations. Still watching yourself blow up over something small and wondering what the hell is wrong with you.
Nothing is wrong with you. But something is definitely still unfinished.
That unfinished business has a name. It’s called emotional sobriety. And it’s the piece of the picture that almost nobody in the mainstream recovery world talks about honestly, because most of what’s out there is either rooted in the 12-step model or so wrapped in clinical language that it’s useless to the person sitting in their kitchen at midnight, sober and still suffering.
This is the honest version.
What Is Emotional Sobriety? The Actual Definition
Emotional sobriety is not about being calm all the time. It’s not about suppressing your feelings, performing wellness, or never raising your voice again. It’s not a personality transplant.
Emotional sobriety is the ability to feel whatever is happening inside you without being run by it.
You can feel the anger and choose how you respond to it. You can feel the fear and still make the call. You can feel the grief and not reach for something to make it stop. You notice the emotion. You observe it. You decide what happens next. The emotion does not decide for you.
That’s it. That’s the whole thing. But getting there from where most people start is serious work.
The term was first used by Bill Wilson, one of the AA founders, in a 1958 letter where he admitted that physical sobriety alone wasn’t enough and that emotional and psychological immaturity was still running the show for many people who hadn’t touched a drink in years. He was right. The problem is that the mainstream recovery world took his insight and pasted it onto the 12-step framework, which means that if you’re not in that world, nobody is giving you a straight answer about what emotional sobriety actually is or how to build it.
The Dry Drunk Problem Nobody Wants to Admit
There’s a term that gets thrown around in recovery circles: the dry drunk. It’s not a kind label, and it’s worth saying upfront that labelling yourself or anyone else a “drunk” of any variety isn’t particularly useful. But the concept underneath the label is real, and it matters.
A dry drunk is someone who has removed the substance but hasn’t dealt with the emotional and psychological patterns that the substance was medicating. They’re not drinking. But the mood swings are still there. The resentment is still there. The emotional volatility, the self-sabotage, the inability to handle stress without blowing the lid off, all of it is still running.
Because the drink was never the root problem, the drink was the solution: a terrible, self-destructive, system-wrecking solution, but a solution to something. When you remove the solution without addressing the thing it was solving, the thing doesn’t disappear. It just runs without its circuit breaker.
I drank for 45 years. I served 12 years in the British Army, where we considered ourselves the fittest, most highly functioning drunks in existence. We were not wrong. I held down a career as an IT technical architect, designing enterprise systems for global organisations. I was analytical, precise, and capable. I could explain every pattern I was running with clinical accuracy.
I was also completely unable to stop.
When I did stop, I hit the dry drunk phase hard. I didn’t know what to call it at the time. I just knew I’d removed the thing I’d used to regulate my nervous system for decades, and now my nervous system was doing whatever it wanted, whenever it wanted, to whoever was nearby. That’s not a recovery story. That’s just a different kind of wreckage.
Emotional sobriety is what comes after. It’s the actual work.
Why Physical Sobriety Is Just the Starting Line
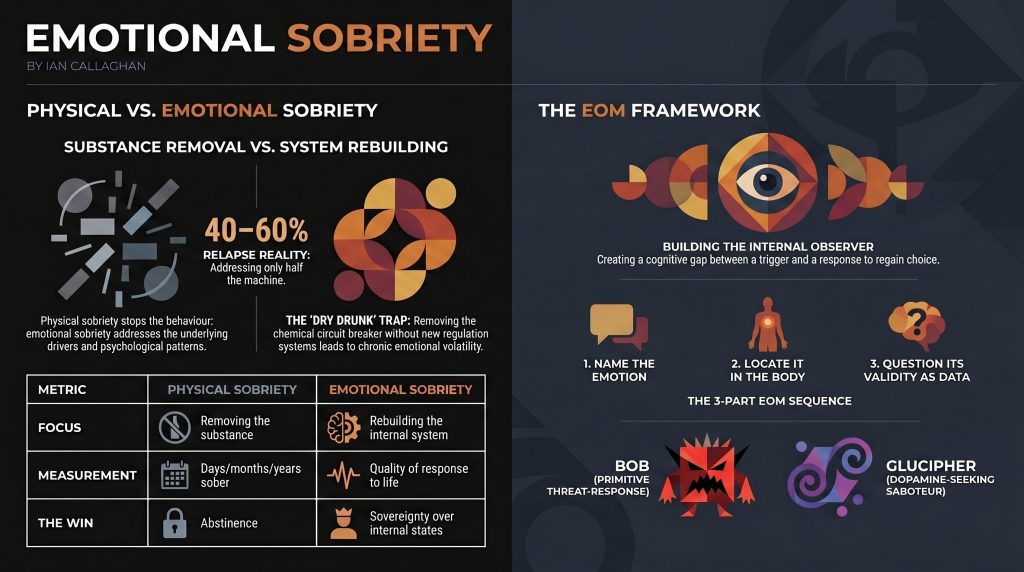
Research consistently shows that somewhere between 40 and 60 per cent of people relapse within the first year of stopping. That’s not a moral failure statistic. That’s a “we’ve only addressed half the machine” statistic.
Here’s what the machine actually looks like.
For most people who use alcohol to cope, the drink is performing several functions at once. It’s regulating a nervous system that never learned to regulate itself. It’s numbing emotional states that feel unbearable or overwhelming. It fills a gap in identity because, without it, you don’t quite know who you are or how to operate socially. It’s medicating unprocessed trauma that has never been named, let alone addressed.
Remove the drink, and all of those underlying functions need somewhere to go. If you don’t build new systems for emotional regulation, the nervous system finds other ways to cope. That might look like food. Work. Rage. Avoidance. Control. Relationships that replicate the same chaos as the old life in a different costume.
Physical sobriety is the starting line. Emotional sobriety is the race.
The Signs You’re Running on Physical Sobriety Alone
This is where it gets uncomfortable. These are the patterns that show up when the drink is gone, but the emotional work hasn’t been done yet. None of them is permanent. All of them are workable. But you have to be honest about recognising them.
Chronic emotional reactivity. Small things hit like big things. Someone cuts you off in traffic, and your day is ruined. A throwaway comment from a colleague and you’re in your head about it for hours. The volume of your response does not match the size of the event.
Resentment that won’t shift. You’re carrying old grievances like they happened this morning. People who wronged you years ago are still living rent-free in your head. You replay old conversations. You construct arguments you’ll never have. You stay angry at things you cannot change.
Shame spirals after emotional outbursts. You lose your temper, you say something you regret, and then you spend three days hating yourself for it. The shame is so familiar it almost feels like home.
Decision paralysis under pressure. When things get stressful, your ability to think clearly disappears. The prefrontal cortex, the brain’s rational decision-making centre, goes offline, and the threat response takes over. You’re running on panic, or you’re frozen. Neither is useful.
Relationship patterns that keep repeating. The people change, but the dynamic stays the same. The same arguments. The same distances. The same feeling that you’re one conversation away from blowing the whole thing up.
Using sobriety itself as an identity rather than a foundation. “I’m a sober person” becomes the whole personality. Every decision runs through that filter. Every social situation is framed around not drinking rather than building something to move toward.
If any of those land, that’s not a judgment. That’s useful information.
Emotional Sobriety vs Physical Sobriety: The Key Differences
Physical Sobriety
Emotional Sobriety
Focus
Removing the substance
Rebuilding the internal system
Measurement
Days/months/years sober
Quality of response to life
The work
Not picking up
Learning to feel without being controlled
What it addresses
The behaviour
The driver of the behaviour
Timeline
Starts day one
An ongoing process, not a destination
Common trap
White-knuckling
Performing emotional wellness
The win
No substance
Sovereignty over your own internal state
Physical sobriety is binary. You either drank or you didn’t. Emotional sobriety is a practice. You’re always somewhere on the spectrum, always capable of moving forward, always capable of slipping backwards, and the measurement isn’t several days. It’s how you navigate the hard moments.
What Emotional Sobriety Actually Feels Like When You’re Building It
This is what nobody tells you: building emotional sobriety is uncomfortable before it gets better. You’re developing the capacity to sit with feelings you’ve spent years running from. That’s not fun. It’s necessary, but it’s not fun.
Here’s what the trajectory looks like.
Early stage: You notice the emotion after the reaction. You’ve already said the thing, sent the message, slammed the door. You look back and see what happened. This is actually progress, even though it doesn’t feel like it. You’re developing the observer. That observer didn’t exist before.
Middle stage: You notice the emotion during the reaction. You can feel yourself being pulled toward the old response. Sometimes you go with it anyway. Sometimes you don’t. The gap between trigger and response is starting to widen.
Building stage: You notice the emotion before you react. The physical sensation in your body, the tightening in your chest, the heat up the back of your neck, you recognise it as data rather than command. You have a choice. You may not always make the right one, but you have a choice.
That progression is not linear, and it’s not quick. But every time you catch it a stage earlier, you’re rewiring something real.
The EOM Framework: Observing Emotions Instead of Being Them
The Emotional Observation Method is the framework I built to close the gap between knowing and doing. Not a therapy model. Not a set of affirmations. A practical system for people who want to understand their own machine well enough to service it differently.
The core principle is deceptively simple: you are not your emotions. You are the one observing them.
When anger arrives, most people fuse with it. They become angry. Every thought is filtered through it. Every decision is made from the inside. Anger is the operating system, and it’s running everything.
EOM creates separation. You notice the anger. You observe it. You ask what it’s telling you. You don’t have to act on it, and you don’t have to suppress it. You listen to it as data, the same way you’d listen to a warning light on a dashboard, and then you decide what to do with the information.
This sounds simple. Doing it when you’re in the middle of a triggered state is another thing entirely. That’s why the practice matters. You don’t build capacity during a crisis. You build it in the quiet moments so it’s available when the crisis arrives.
The three-part EOM sequence:
Name it. Give the emotion an actual label. Not “I’m stressed” but “I’m feeling afraid that I’m going to lose control of this situation.” Specificity matters. Research from UCLA shows that naming an emotion reduces amygdala activation, meaning it literally turns down the volume on the threat response.
Locate it. Find it in your body. Emotions are not abstract. They live somewhere. The tightness in the throat. The weight in the chest. The heat in the jaw. Finding the physical location gives you something concrete to work with.
Question it. What is this emotion actually responding to? Is this a real threat or an old pattern firing on a new trigger? Is the size of this response proportionate to the actual situation? What does this emotion want me to do, and is that the right move?
That three-part sequence, practised consistently, starts to build the observer. And once the observer is strong enough, you have something to work with.
Bob, Glucipher, and the Characters Running Your Emotional Show
Within the EOM framework, I use two characters to explain the forces driving emotional reactivity. Not to make it cute. Because understanding what’s driving the pattern is the first step to not being driven by it.
Bob is your inner chimp. Your primitive threat-response machine. Bob has been keeping you alive since you were born. Bob’s job is to protect you from danger, social exclusion, loss of status, and anything that reminds him of past pain. Bob is fast, loud, and completely uninterested in what’s actually appropriate in a 21st-century conversation. When you lose your temper at a minor inconvenience, Bob is behind it. When you interpret a neutral comment as an attack, Bob is behind it. Bob is not your enemy. But Bob should not be in charge.
Glucipher is the blood sugar and dopamine saboteur. The part of the system that has learned to crave quick relief and will pitch whatever story is necessary to get it. When the emotional discomfort gets high enough, Glucipher starts building the case for why a drink makes sense, why comfort eating makes sense, why staying in bed makes sense, and why burning the relationship to the ground makes sense. Glucipher is a brilliant storyteller and a terrible strategist.
Emotional sobriety is not about silencing Bob or destroying Glucipher. It’s about making sure neither of them is driving the car.
7 Practical Ways to Build Emotional Sobriety Without a Programme
These are not affirmations. These are not things you put on a vision board. These are practices that build genuine neurological change over time.
1. Regulate the nervous system first, everything else second.
You cannot build emotional sobriety on a dysregulated nervous system. This is non-negotiable. For me, that means daily cold-water exposure in the River Usk year-round, daily meditation, Reiki practice, and OMAD eating, which keeps blood sugar stable and eliminates the spikes and crashes that Glucipher feeds on. Your version will look different. But the nervous system work comes first. Before the journaling, before the therapy, before any of it.
2. Build the observer through daily stillness.
Meditation is not about emptying your mind. It’s about practising being the one watching the mind rather than being the mind. Even ten minutes a day of sitting with your thoughts without acting on them builds the observer muscle. That muscle is what gives you the gap between trigger and response.
3. Get honest about your emotional triggers.
Write them down—the specific situations, people, topics, and dynamics that reliably pull you into reactive states. Most people have six to ten consistent triggers. Once you can see them on paper, they lose some of their power to operate in the dark.
4. Track your physical state.
Tired, hungry, pain, alcohol withdrawal in early sobriety, all of these narrow your emotional window dramatically. A narrow emotional window means smaller triggers produce bigger reactions. Tracking how physical state affects emotional reactivity gives you predictive information you can actually use.
5. Learn the difference between responding and reacting.
A reaction is immediate, automatic, and driven by the threat system. A response involves a pause, however brief, between stimulus and action. The practice is extending that pause. One breath before you reply to the email. One moment before you walk back into the room. Tiny pauses, practised consistently, become a real capacity.
6. Stop outsourcing emotional regulation.
If you’ve spent years using alcohol to regulate your emotional state, you’ve been outsourcing that regulation to a chemical. The work of emotional sobriety is bringing it back in-house. That means developing internal tools, breathwork, cold exposure, movement, stillness, and using them when the pressure is on rather than waiting for someone or something outside yourself to make you feel better.
7. Get comfortable with discomfort without escaping it.
This is the core skill underneath everything else. Emotions are not emergencies. Discomfort is not a crisis. You can feel terrible and not act on it. You can be angry and not express it destructively. You can be afraid and still do the thing. The capacity to sit with discomfort without immediately moving to escape it is the foundation on which everything else rests.
Emotional Sobriety and Men: The Stoic Mask Problem
Most men are never taught that emotions are information. They’re taught that emotions are a weakness. They’re taught to suppress, to perform invulnerability, to identify strength with never showing anything that could be mistaken for feeling.
That conditioning doesn’t just disappear when you get sober. In some cases, sobriety makes it worse, because the one mechanism you’d been using to avoid feeling anything has been removed, and now the feelings are just there, with nowhere to go and no permission to be acknowledged.
The result is men who are physically sober and emotionally constipated. The anger comes out sideways. The grief becomes resentment. The fear becomes control. And the people around them cope with the fallout of feelings that have never been named, never been processed, and never been given a useful direction.
Emotional sobriety for men is not about becoming someone who talks about feelings in groups. It’s about developing enough internal intelligence to know what you’re actually experiencing, make your own decisions about how to handle it, and stop letting unexpressed emotion run your life through the back door.
I spent 12 years in the British Army. I know what the culture expects. I also know what it costs in the long term to pay that price. The herniated discs at L3, L4, and L5 that I carry from my service are a physical reminder of what happens when a machine is run past its limits without servicing. The emotional equivalent is nonetheless damaging. It just shows up more slowly.
How Trauma Keeps Emotional Sobriety Out of Reach
If emotional sobriety feels impossible, no matter how much you try, trauma may be the reason.
Trauma is not just catastrophic events. Trauma is any experience that overwhelmed your nervous system’s capacity to process it at the time it happened. Childhood emotional neglect. A relationship that systematically dismantled your sense of reality. Military service that asked you to process the unprocessable with no real support. Years of shame-based living that taught your system that emotions themselves are dangerous.
Unprocessed trauma creates a state of chronic nervous system dysregulation. Your threat system is permanently calibrated too high because it learned, at some point, that the world is not safe enough to relax in. Emotions arrive at elevated volume and with compressed response timeframes. The window of tolerance is narrow.
No amount of willpower closes that gap. You’re not going to think your way out of a nervous system that has been shaped by experience. You need approaches that work at the level where the damage happened.
For me, that combination includes NLP for reprogramming unconscious patterns, Reiki for working with the energetic and emotional body, cold water immersion for direct regulation of the nervous system, and consistent daily practices that help keep the system in a more regulated state over time. What works for you may look different. But if trauma is in the picture, the path to emotional sobriety runs through it, not around it.
For anyone whose emotional reactivity feels completely outside their control, the deep dive is in the self-sabotage framework in Under Load, specifically the section on the system under pressure.
The Connection Between Emotional Sobriety and Physical Health
This is where things get interesting for anyone paying attention to both their body and their mind.
Chronic emotional dysregulation is not just a psychological problem. It’s a physiological one. Sustained activation of the stress response elevates cortisol, suppresses immune function, disrupts sleep, drives inflammatory processes, destabilises blood sugar, and degrades the quality of every system in the body.
If you’re working on your metabolic health, your sleep, your gut, and your energy while ignoring the emotional regulation piece, you’re leaving a significant variable unaddressed. The body and the nervous system are not separate departments. They’re one system.
This is why the midlife reset work covers all four pillars: eat, sleep, move, and mind. You cannot genuinely optimise one without addressing the others. Emotional sobriety sits inside the mind pillar, but its effects run through the entire machine.
Cold water immersion, which has been part of my practice for decades in the River Usk, is one of the most direct tools available for nervous system regulation. Vagus nerve stimulation from cold exposure builds the same capacity to tolerate discomfort that emotional sobriety requires. You’re training the same system.
What Emotional Sobriety Is Not
It’s worth clearing up some misunderstandings because they actively prevent people from doing the work.
It is not about never feeling negative emotions. Anger, grief, fear, disappointment, these are not failure states. They’re appropriate responses to real events. Emotional sobriety doesn’t mean the emotions disappear. It means they do not control you.
It is not about performing positivity. The wellness industry has a version of emotional health that involves gratitude journals, manifesting, and relentlessly reframing everything as a blessing. That’s not emotional sobriety. That’s emotional suppression with better branding.
It is not a weakness. The person who can sit with emotional discomfort without immediately discharging it into the environment is not weak. They are practising a form of self-mastery that most people never develop because they were never shown it was possible.
It is not a destination. You don’t arrive at emotional sobriety and stay there. It’s an ongoing practice. You will have days when you handle things well and days when you don’t. The measurement is not perfect. It’s the direction of travel.
It is not the same as suppression. Suppression is forcing the emotion down and not letting it surface. That’s the old model, the stoic mask, the “man up” default. Suppression stores what it can’t process. Emotional sobriety is the opposite: you feel the emotion fully and choose what to do with it.
Emotional Sobriety and the Sober Beyond Limits Community
In the Sober Beyond Limits community, this is one of the most consistent themes that comes up from people who are months or years into not drinking and still struggling with why life doesn’t feel the way they thought it would.
Physical sobriety is the entry point. What builds after it determines the quality of the life you’re actually living.
The conversations in that space are not about milestones and chips. They’re about the real work of becoming someone who doesn’t need the drink, because the underlying reasons to reach for it have been addressed. That’s a different project from counting days. It’s a harder project and a more worthwhile one.
If you’re sober and still suffering, that’s not a sign you’ve failed. It’s a sign there’s a next stage of work available to you.
A Note on Professional Support
The work described in this post is real, and it’s doable. It’s also not always work you should do alone.
If your emotional reactivity is severe, if there’s significant trauma in your history, if you’re experiencing what looks like depression or anxiety alongside the reactivity, getting proper support matters. Not because you can’t handle it, but because having the right tools for the specific job makes everything more effective.
What doesn’t matter is which label you carry or which programme you’re part of. The work is the work. The framework is secondary to whether you’re actually doing it. If the 12-step model works for you, use it. If it doesn’t, there are other paths. What’s not an option is staying stuck in a life where you’re physically sober and emotionally wrecked and calling that the destination.
For people dealing with the darker end of this, the piece on suicidal thoughts and what actually helped is honest about what rock bottom with a functioning sobriety looks like, and what came after.
Frequently Asked Questions About Emotional Sobriety
What is the difference between emotional sobriety and physical sobriety?
Physical sobriety means you have stopped using the substance. Emotional sobriety means you have developed the internal capacity to manage your emotional states without reaching for a substance or any other external fix. Physical sobriety is the first step. Emotional sobriety is the deeper work that makes the first step sustainable and actually worth living.
Can you have emotional sobriety without being physically sober?
Technically,y yes, in the sense that emotional regulation is a skill that anyone can develop. But in practice, if you’re still actively drinking, the neurological and physiological effects of alcohol on the brain’s emotional regulation systems make genuine progress extremely difficult. The nervous system’s work becomes exponentially harder when the substance continues to disrupt it.
How long does it take to develop emotional sobriety?
There is no timeline. It’s a practice, not a course. Most people start noticing meaningful shifts in their emotional reactivity within three to six months of consistent work. Deeper patterns, especially those rooted in trauma, take longer. The honest answer is that it’s ongoing, and the goal is progress in the right direction, not completion.
Is emotional sobriety possible without therapy?
Yes, though therapy can accelerate the process significantly, particularly for people with significant trauma in their history. Consistent practice of emotional regulation tools, nervous system regulation, honest self-inquiry, and community support can build emotional sobriety without formal therapy. But if you’re stuck, or if the emotional reactivity is severe, getting professional support is not a failure. It’s a sensible use of available tools.
What does emotional sobriety feel like in practice?
It feels like having a gap. A pause between something happening and your response to it. That gap feels small at first, almost imperceptible. Over time, it grows. You start to notice that you can feel the anger without becoming it, feel the fear without being paralysed by it, feel the grief without drowning in it. Life doesn’t become easy. You become better at handling it.
I’ve been sober for years, but I’m still emotionally reactive. Is this normal?
Yes. Physical sobriety does not automatically produce emotional sobriety, and the length of time you’ve been sober is not a reliable indicator of where you are in the emotional work. Plenty of people with significant sobriety milestones are still running the same emotional patterns they were running in active use. The duration of sobriety matters less than whether the underlying work has been done.
Does emotional sobriety apply to people who don’t have a drinking problem?
Entirely. Emotional sobriety is a life skill, not a recovery concept. Anyone who finds themselves regularly controlled by their emotional states, making decisions from within reactive states they later regret, or using external fixes to regulate internal discomfort is dealing with the same territory. The drink is the most visible version of the problem. It’s not the only version.
What is the Emotional Observation Method?
The EOM is a framework developed from lived experience, NLP, and nervous system work that creates a practical system for observing emotions rather than being run by them. It’s built around the principle that you are not your emotions: you are the one observing them. The core practice is building the observer: the internal capacity to notice what’s happening in your emotional system and make a considered choice about what to do with it, rather than defaulting to an automatic reaction.
The Bottom Line on Emotional Sobriety
You stopped drinking. That was the starting line, not the finish line.
Emotional sobriety is the work that happens after. It’s building an internal system that doesn’t need the drink because the underlying reasons for reaching for it have been addressed. It’s developing the capacity to feel whatever life throws at you without it running you. Over time, it’s becoming someone who operates from choice rather than reaction.
That’s not a wellness retreat concept. That’s the actual job.
Nobody does it perfectly, and nobody arrives at the destination and stays there. But the direction of travel matters enormously. Every time you catch the emotion one stage earlier, every time you choose response over reaction, every time you sit with the discomfort instead of escaping it, you’re building something that compounds.
The machine runs better when it’s been properly serviced. That’s what this work is. Not a cure, not a transformation, not a new identity. Just a properly serviced machine, doing what it was built to do.
If you’re ready to go deeper into the framework, the Under Load self-sabotage book paints the full picture of why intelligent, self-aware people keep repeating patterns that destroy them, and what the systems-based alternative actually looks like.
And if you’re in the middle of this work and want to be around people who are doing it seriously, without the milestones, without the labels, without the programme language, the Skool community at Ian Callaghan Midlife Reset is where that conversation happens.
Pick up the wrench. 🔧
Ian Callaghan is a British Army veteran (12 years), NLP Master Practitioner, Reiki Master, qualified chef, and creator of the Emotional Observation Method. He spent 45 years drinking and did not use AA, rehab, or any programme to stop. He works with people who want to understand their machine well enough to service it differently. Find him at iancallaghan.co.uk.
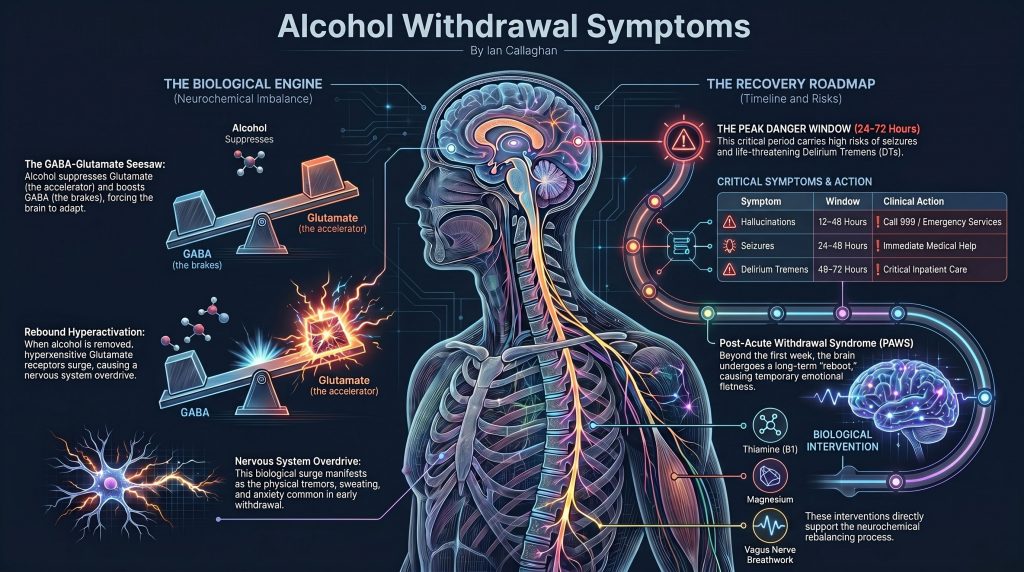
Alcohol withdrawal symptoms occur when the brain’s chemical balance is disrupted after stopping or significantly reducing alcohol. They typically begin 6 to 12 hours after the last drink and include anxiety, tremors, sweating, nausea, and insomnia. Symptoms peak between 24 and 72 hours. Severe symptoms — including seizures and delirium tremens — can be life-threatening and require immediate medical attention. Alcohol withdrawal happens because chronic drinking forces the brain to adapt its neurotransmitter systems. When alcohol is removed, those adaptations cause a rebound of neurological hyperactivity. This is a medical event, not a character failing.
Author: Ian Callaghan | Reiki Master | Sobriety and Nervous System Coach | Author of Under Load and Sober Beyond Limits | 45 years of lived experience with alcohol | Monmouthshire, UK
Introduction
You stopped drinking.
Maybe last night. Maybe three days ago. Maybe you’re planning to stop tonight, and you want to know what’s coming.
Either way, your body is doing something right now that nobody has properly explained to you. Not the NHS leaflet. Not the AA pamphlet. Not the well-meaning person who told you to drink more water and get an early night.
This is what’s actually happening — the mechanism, the timeline, the symptoms that are uncomfortable but normal, and the ones that mean you need medical help immediately.
No judgment. No agenda. Just the biology.
I am Ian Callaghan. I drank for 45 years. I know this territory from both sides — from the inside, and from the science I went looking for when I finally needed to understand what my body had been doing all that time.
If you want to understand how dangerous withdrawal can be before reading further, I have written a dedicated piece on exactly that: how dangerous are alcohol withdrawals when you stop drinking. This post covers the full neuroscience and mechanism underneath it.
What Are Alcohol Withdrawal Symptoms?
Alcohol withdrawal symptoms are the physical and psychological effects that occur when someone who has been drinking heavily stops or significantly reduces their alcohol intake.
They happen because alcohol is not just a drink. It is a central nervous system depressant that, over time, physically restructures the way your brain regulates itself. When you remove it, the brain doesn’t simply return to normal. It overshoots in the opposite direction.
The result is a nervous system in temporary overdrive — anxious, hyperactivated, and struggling to rebalance without the chemical it has been built around.
Why Does Alcohol Withdrawal Happen? The Brain Chemistry Explained
What Alcohol Does to Your Brain Over Time
Your brain runs on a careful balance between two primary neurotransmitters.
GABA — gamma-aminobutyric acid — is your brain’s braking system. It slows neural activity, reduces anxiety, and promotes calm and relaxation.
Glutamate is your brain’s accelerator. It drives alertness, energy, excitation, and cognitive arousal.
In a healthy brain, these two systems hold each other in check. The balance between them determines how activated or calm your nervous system runs at any given moment.
Alcohol hijacks this system. Every drink artificially boosts GABA and simultaneously suppresses glutamate. That is why alcohol feels the way it does — the brakes come on, the accelerator goes quiet, you relax, your inhibitions drop, and your anxiety reduces.
But your brain is not passive. It is constantly trying to maintain homeostasis — balance. And it adapts to the repeated chemical override.
Over weeks, months, and years of regular drinking, the brain compensates. It downregulates GABA receptors, reducing their sensitivity. It upregulates glutamate receptors, making them hypersensitive. It is literally rebuilding its architecture around the alcohol, fighting to keep functioning normally despite the repeated chemical suppression.
This is why tolerance develops. This is why you need more to feel the same effect. And this is why stopping creates a crisis.
For a deeper breakdown of the full neurochemical picture — dopamine, serotonin, endorphins, and the reward system — read: The Brain Chemistry of Addiction.
What Happens When You Stop Drinking Alcohol
When you stop drinking, the alcohol leaves your system. But the receptor changes your brain made do not reverse overnight.
You are now sitting with weakened brakes and a hypersensitive accelerator — with nothing suppressing the system.
Glutamate surges. GABA cannot contain it. The nervous system goes into rebound hyperactivation.
That is alcohol withdrawal. A predictable neurological event with a known mechanism, a measurable timeline, and a clear set of inputs that either help or harm the recovery process.
What Happens to Your Body When You Stop Drinking Alcohol: The Full Timeline
Severity varies significantly based on the length and volume of drinking, individual neurobiology, and overall health. This is the general clinical map.
Hours 6–12: The First Wave Begins
Within six to twelve hours of the last drink, the rebound begins.
This is the initial glutamate surge. The nervous system is in early hyperexcitation. Uncomfortable, but not dangerous at this stage for most people.
Hours 12–48: Peak Intensity
This is the hardest window for most people withdrawing from alcohol.
Symptoms at this stage:
Worsening anxiety, potentially severe
Pronounced tremors
Profuse sweating
Elevated blood pressure and heart rate
Complete inability to sleep
Hypersensitivity to light and sound
Severe emotional instability — fear, rage, grief without a clear trigger
In 2–8% of cases: hallucinations — auditory, visual, or tactile
If you are hearing voices, seeing things, or feeling sensations on your skin that are not there, this is a medical emergency. Call emergency services.
Hours 24–72: The Danger Window
Withdrawal seizures occur in up to 15% of people going through significant alcohol withdrawal, typically between 12 and 48 hours after the last drink. They can happen with no preceding warning signs. They are major motor seizures — full body convulsions.
If a seizure occurs: call emergency services immediately. Do not wait.
Delirium tremens (DTs) — the most severe form of alcohol withdrawal — typically emerges between 48 and 72 hours, though it can appear up to seven days after stopping. It affects 3–5% of people withdrawing from alcohol.
Symptoms of delirium tremens include:
Severe confusion and disorientation
Agitation and aggression
High fever
Rapid, irregular heartbeat
Profuse sweating
Hallucinations
Seizures
Without treatment, delirium tremens can be fatal. With prompt medical intervention, survival rates are high. This is why medical supervision during high-risk withdrawal is not optional.
You are at higher risk of severe withdrawal if:
You have been drinking heavily daily for months or years
You have experienced withdrawal before, particularly if it was severe
You have previously had a withdrawal seizure
You have liver disease, heart conditions, or other significant health conditions
You are stopping abruptly after a very high daily consumption
If any of these apply, speak to a doctor before stopping. Read the full breakdown of risk factors here: How dangerous are alcohol withdrawals when you stop drinking?
Days 4–7: The Climb Down
For most people without severe complications, symptoms begin to ease after 72 hours. The acute glutamate surge starts to settle. GABA receptor sensitivity begins to recover.
Sleep remains disrupted. Anxiety continues at a lower level. Brain fog, physical fatigue, and emotional flatness are common. But the acute danger window has passed for most people.
Beyond Day 7: Post-Acute Withdrawal Syndrome (PAWS)
This is the part nobody tells you about. And the part that derails more recoveries than the acute phase ever does.
For many people — particularly those who drank heavily for years — a subtler, longer withdrawal phase follows the acute period—clinically referred to as post-acute withdrawal syndrome, or PAWS.
PAWS symptoms can include:
Persistent sleep disruption — weeks or months of broken, unrefreshing sleep
Cognitive fog — slow thinking, poor concentration, difficulty retaining information
Anhedonia — the inability to feel pleasure or motivation from things that previously provided it
Cravings arrive in waves, often triggered by stress, poor sleep, or emotional states
Low energy and flat affect that feels indistinguishable from depression
The anhedonia piece catches most people completely off guard. If sobriety feels grey, flat, and pointless — that is not a sign that you were better off drinking. That is your dopamine system rebooting after years of chemical override. Read the full breakdown: anhedonia in early sobriety.
The gut-brain axis is also a key driver of PAWS that most withdrawal conversations completely ignore. Chronic alcohol use devastates the gut microbiome, which directly impacts neurotransmitter production, mood regulation, and the stress response. The nervous system cannot fully stabilise while the gut remains dysbiotic. This is not a side issue — it is central to why PAWS drags on—full explanation here: gut-brain axis and alcohol recovery.
GABA and glutamate function largely normalises within one to three months. Dopamine and serotonin systems take longer. Research suggests full neurochemical normalisation can take up to a year or more for long-term heavy drinkers.
This is not permanent damage in most cases. It is a healing process with a timeline.
Understanding that the flatness, the fog, and the low mood are mechanistic — that they are your brain rebuilding, not evidence that sobriety feels worse than drinking — changes everything about how you move through it.
What Helps During Alcohol Withdrawal: The Biology of Recovery
These are not wellness suggestions. These are inputs that directly support the neurochemical rebalancing process.
Hydration and Electrolytes
Sweating during withdrawal rapidly depletes sodium, potassium, and magnesium. Water alone does not replace them. Electrolyte-rich fluids, broth, and real food, which are tolerable, support the cellular environment the nervous system needs to repair.
Magnesium is directly involved in GABA receptor function and nervous system regulation. It is aggressively depleted by chronic alcohol use. Supplementing during and after withdrawal — magnesium glycinate or citrate for absorption — directly supports the GABA recovery process.
B Vitamins — Particularly Thiamine (B1)
Alcohol depletes thiamine at an extreme rate. Thiamine deficiency during withdrawal can cause Wernicke’s encephalopathy — a serious neurological complication involving confusion, coordination problems, and vision changes. B complex supplementation in the early days of cessation is protective, not optional. If in any doubt, speak to a doctor about injectable thiamine.
Breathwork — The Vagus Nerve Mechanism
The glutamate surge drives sympathetic nervous system dominance — the fight-or-flight state running at full activation. Extended exhale breathing — where the exhale is longer than the inhale — directly activates the vagus nerve and shifts the autonomic nervous system toward parasympathetic dominance.
This is not relaxation advice. This is a direct mechanical intervention on the nervous system hyperactivation, driving withdrawal symptoms.
A simple starting point: inhale for four counts, exhale for six to eight. Five minutes. Notice what shifts.
The vagus nerve is the biological mechanism underneath this. For a full explanation of how it works and why it matters in recovery: vagus nerve and mental health. And specifically, how the vagal brake functions as your nervous system’s self-regulation switch.
Cold Water Exposure
Brief cold showers or cold water immersion create a controlled acute stress response that, when repeated, trains the nervous system back toward regulation. The initial shock, followed by the physiological adaptation, builds vagal tone — the nervous system’s capacity to self-regulate. Start with thirty seconds at the end of a normal shower and build from there.
The brain does the majority of its repair and neurotransmitter synthesis during sleep. Keep the environment dark, cool, and free of screens. Even lying still with eyes closed — without full sleep — allows the nervous system to recover partially.
Do not use alcohol to sleep. The sedation it creates is not restorative sleep. It actively prevents REM and deep sleep stages, during which neurological repair occurs.
Gentle Movement
Rhythmic movement — walking, slow bodyweight exercises — helps clear elevated cortisol and stress hormones and supports the production of endorphins and dopamine through natural pathways. Do not push through exhaustion. Move enough to shift the chemical state without depleting what little reserve you have.
When To Get Medical Help — No Ambiguity Here
Call 999 or go to A&E immediately if you experience:
Seizures or convulsions of any kind
Severe confusion or disorientation — not knowing where you are or what is happening
Hallucinations — seeing, hearing, or feeling things that are not there
High fever combined with agitation
Extremely rapid or irregular heartbeat
Loss of consciousness
Speak to a doctor before stopping drinking if:
You have been drinking heavily daily for more than a few weeks
You have withdrawn before, and it was severe or involved seizures
Do you have any existing medical conditions, particularly heart or liver-related
Are you on any medications that may interact with withdrawal
Do not attempt to manage high-risk withdrawal alone. Medical supervision and, where necessary, medication make this significantly safer. That is a clinical fact, not a judgment on your capacity to cope.
How to Stop Drinking Alcohol: What Comes After the Acute Phase
Getting through withdrawal is the beginning, not the end.
The nervous system that was built around alcohol does not simply reset when the acute symptoms resolve. The reward circuitry, the stress response architecture, the gut-brain communication pathways — all of them were shaped by years of chemical intervention. All of them need deliberate rehabilitation.
The work that comes after acute withdrawal — rebuilding GABA naturally, restoring gut-brain axis function, recalibrating the stress response, rebuilding dopamine pathways through earned reward rather than chemical shortcut — is where most people either find solid ground or relapse back into the same loops.
If you are quitting cold turkey, read this first: Quitting Cold Turkey — The Risks, the Reality, and How to Do It as Safely as Possible.
That is the work. And it is available to anyone willing to approach it with the right information.
FAQ: Alcohol Withdrawal Symptoms
How long do alcohol withdrawal symptoms last? Acute alcohol withdrawal symptoms typically begin within 6 to 12 hours of the last drink, peak between 24 and 72 hours, and resolve for most people within 5 to 7 days. However, post-acute withdrawal syndrome (PAWS) can persist for weeks to months, with symptoms including sleep disruption, mood instability, cognitive fog, and cravings.
What are the first signs of alcohol withdrawal? The first signs of alcohol withdrawal typically appear 6 to 12 hours after the last drink and include anxiety, hand tremors, sweating, headache, nausea, elevated heart rate, and insomnia. These early symptoms reflect the initial GABA-glutamate rebound in the brain.
Can alcohol withdrawal kill you? Yes. Severe alcohol withdrawal can be fatal without medical intervention. Delirium tremens — which affects 3 to 5% of people withdrawing from alcohol — can cause fatal cardiovascular and neurological complications if untreated. Withdrawal seizures, which occur in up to 15% of significant withdrawal cases, also carry risk. Anyone at high risk of severe withdrawal should seek medical supervision before stopping.
What happens to your body when you stop drinking alcohol? When you stop drinking alcohol, your brain enters a rebound state. The GABA system — suppressed by chronic alcohol use — becomes underactive. The glutamate system — also chronically suppressed — rebounds into hyperactivity. This neurological imbalance produces the physical and psychological symptoms of withdrawal. Over days to weeks, the brain begins to rebalance its neurotransmitter systems and restore natural regulation.
What is the difference between a hangover and alcohol withdrawal? A hangover is the acute aftermath of a single drinking session — dehydration, acetaldehyde toxicity, disrupted sleep, and a mild GABA-glutamate rebound. Alcohol withdrawal is a distinct medical condition that occurs in people with physical dependence on alcohol, where the brain has structurally adapted to alcohol’s presence and cannot function normally without it. Withdrawal symptoms are more severe, more prolonged, and potentially life-threatening in a way that a hangover is not.
What is alcohol cessation syndrome? Alcohol cessation syndrome is another term for alcohol withdrawal syndrome — the collection of physical and neurological symptoms that occur when a person who is physically dependent on alcohol stops or reduces their intake. It ranges from mild anxiety and tremors to potentially fatal complications, including seizures and delirium tremens.
How do you stop drinking alcohol every night safely? If you drink heavily every night and want to stop, the safest approach is to speak to a doctor first. For mild dependence, a gradual reduction may be appropriate. For moderate to severe dependence, medically supervised detox reduces the risk of serious complications. After the acute phase, the focus shifts to nervous system rehabilitation — rebuilding natural regulation through nutrition, sleep, breathwork, movement, and gut-brain axis recovery.
Why do I feel anxious and shaky after stopping drinking? Anxiety and shakiness after stopping drinking are direct symptoms of the GABA-glutamate rebound. Alcohol artificially boosted GABA (the calming neurotransmitter) and suppressed glutamate (the excitatory neurotransmitter) during drinking. When alcohol is removed, glutamate surges back while GABA remains underactive, creating a state of neurological hyperexcitation that manifests as anxiety, tremors, and physical agitation.
Does alcohol withdrawal get worse each time? Yes, in many cases. This is known as the kindling effect — each episode of withdrawal can sensitise the brain’s excitatory systems, making subsequent withdrawals more severe. This is one of the key reasons why medically supervised management of withdrawal is important, particularly for anyone who has withdrawn multiple times before.
What is post-acute withdrawal syndrome (PAWS)? Post-acute withdrawal syndrome (PAWS) is the prolonged phase of withdrawal that follows the acute stage. It can last weeks to months and includes symptoms such as persistent insomnia, mood instability, cognitive fog, anhedonia, and intermittent cravings. PAWS is driven by the slow rebalancing of neurotransmitter systems — particularly dopamine and serotonin — and the ongoing recovery of the gut-brain axis after years of alcohol-related damage.
The Bottom Line on Alcohol Withdrawal Symptoms
Alcohol withdrawal is your nervous system reclaiming itself.
It is painful. In some cases, it is dangerous. But what is happening underneath — the GABA receptor recovery, the glutamate settling, the slow return of natural dopamine and serotonin regulation — is your brain learning to function again without a chemical it was built around.
The acute phase ends. The fog begins to lift. The flatness gives way — not all at once, but incrementally, measurably, if you give the biology the right conditions to complete the work.
Most people who relapse do so not during acute withdrawal but during the weeks that follow — when the brain’s reward system is still offline, when sleep is still broken, when the reasons they drank are still present, but the chemical relief is gone.
That gap is where the real work lives. And it has a framework.
If you are in the early days and want to understand the full neurological picture of what comes after withdrawal — and what the rebuild actually looks like:
This article is for informational purposes only and does not constitute medical advice. If you are experiencing severe alcohol withdrawal symptoms, contact emergency services or your doctor immediately. Alcohol withdrawal can be life-threatening. You do not have to manage it alone.
Ian Callaghan is a sobriety coach, Reiki Master, and author based in Monmouthshire, Wales. He writes from 45 years of lived experience with alcohol and a decade of research into the neuroscience of addiction and recovery.
By Ian Callaghan | Nutritional Strategist | Author of Fix Your Metabolism & The 30-Day Reset | Gut Brain Neurodegeneration
“The day I understood that neurodegeneration begins in the gut — not the brain — was the day everything changed. Not just what I ate. How I thought about ageing, about disease, about the decades I had ahead of me.”
What Nobody Is Telling You About Brain Disease and Gut Brain Neurodegeneration
Gut Brain Neurodegeneration. Here is a question your GP has almost certainly never asked you.
How’s your gut?
Not because they don’t care. But because in five-plus years of medical training, the average UK GP receives less than one week of total education on nutrition and gut health. One week. It covers the system that produces 90% of your serotonin, 50% of your dopamine, and houses more neurons than your entire spinal cord.
That blind spot is costing people their minds. Literally.
Because the science — published in leading neuroscience journals, studied at Stanford, and presented at the highest levels of academic research in 2025 — is telling us something that changes everything we thought we knew about brain disease.
Parkinson’s doesn’t start in the brain. It starts in your gut.
Alzheimer’s isn’t a memory disease. It’s a metabolic one.
Neurodegeneration isn’t inevitably bad luck. It’s a downstream consequence of a gut environment that’s been quietly failing for decades.
This is the definitive guide to understanding the gut-brain highway, how it works, and how it breaks. And what you can do, starting today, to protect your neurological future.
The Architecture of the Gut-Brain Axis: What You Were Never Taught
Your gut and your brain are in constant conversation. Not metaphorically. Physically. Through a sophisticated bidirectional communication network called the Gut-Brain Axis (GBA).
This network operates through three primary channels:
Neural — Direct physical connection via the vagus nerve, the longest nerve in your autonomic nervous system
Humoral — Chemical signals sent through the bloodstream, including hormones and metabolites
Immune — The systemic movement of inflammatory cytokines and immune cells
The gut contains its own nervous system — the Enteric Nervous System (ENS) — embedded within the lining of the gastrointestinal tract. It has more than 500 million neurons. It operates with remarkable autonomy. Scientists call it the Second Brain.
And here is the architectural detail that most people miss entirely.
The vagus nerve — the physical highway connecting your gut to your brainstem — is composed of 80% afferent (sensory) fibres. That means the overwhelming majority of traffic along this nerve flows upward. Bottom-up. From your gut to your brain.
Your brain is not commanding your gut. Your gut is reporting to your brain. Constantly. Every hour of every day. Based on what you feed it.
When the report is good — a diverse microbiome, a strong gut lining, and healthy SCFA production — your brain receives signals of safety, repair, and neurological protection.
When the report is bad — dysbiosis, leaky gut, bacterial endotoxins — your brain receives alarm signals that trigger inflammation, accelerate protein misfolding, and set the conditions for the slow-motion catastrophe we call neurodegeneration.
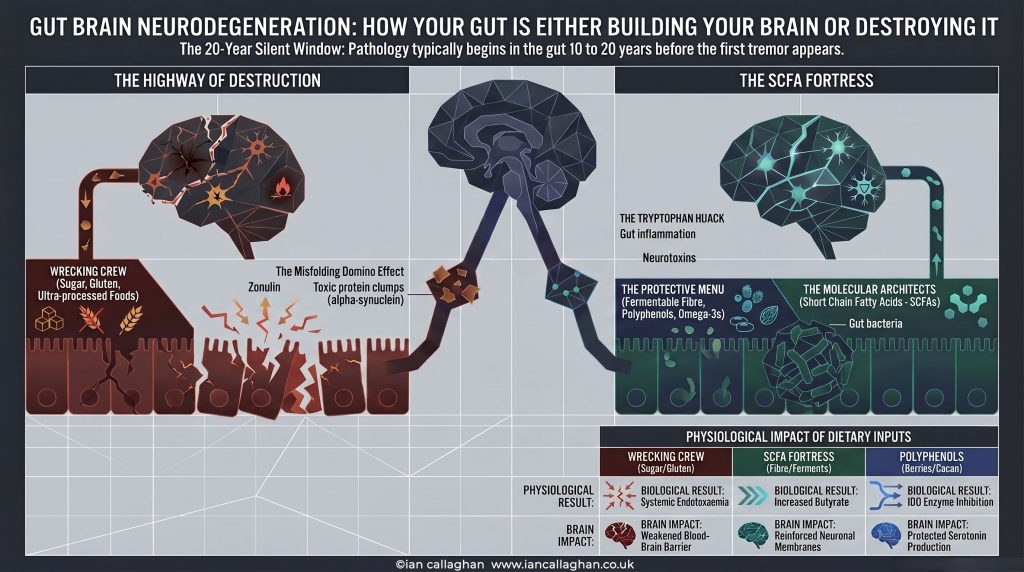
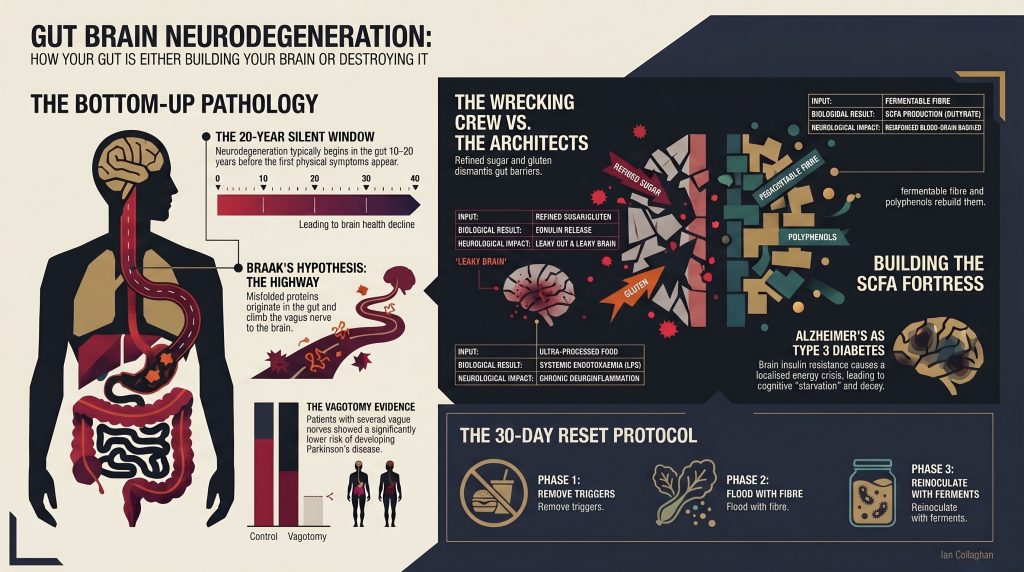
The 20-Year Silent Window: When Disease Begins Long Before Symptoms Appear
This is the part that should stop you in your tracks.
By the time a Parkinson’s patient experiences their first tremor — the shaking hand, the shuffling gait, the rigidity that changes a life overnight — the pathological process that caused it has typically been running for 10 to 20 years.
Two decades. Silent. Invisible. Building in the gut wall before the first symptom ever reaches the brain.
This is what Braak’s Hypothesis tells us. And the evidence behind it is compelling enough to have fundamentally shifted how the world’s leading neuroscientists think about disease prevention.
The implication is enormous.
If the disease starts in the gut, and the disease starts 10 to 20 years before diagnosis, then the intervention window — the period during which you can actually change the trajectory — isn’t at diagnosis. It’s right now. Decades before any neurologist ever entered the picture.
What you eat today is either building the conditions for future neurological health or quietly laying the groundwork for disease. Not as a metaphor. As a biological mechanism.
Braak’s Hypothesis: The Science That Changes Everything
In 2003, German neuroanatomist Heiko Braak proposed something that the medical establishment largely ignored for years. He suggested that Parkinson’s disease doesn’t originate in the substantia nigra — the brain region whose dopamine-producing neurons are destroyed in the disease — but in the gut’s enteric nervous system.
The mechanism he proposed goes like this.
Step 1 — The Trigger in the Gut
Environmental triggers — pesticides, bacterial toxins called lipopolysaccharides (LPS), heavy metals — breach a compromised gut lining and enter the enteric nervous system. Here, they cause a protein called alpha-synuclein to misfold. In its healthy state, alpha-synuclein is soluble and harmless. Under inflammatory stress, it changes shape. It becomes sticky. It aggregates into toxic clumps.
Step 2 — The Prion-Like Spread
These misfolded protein clumps don’t stay put. They behave almost like prions — corrupting healthy proteins around them in a domino effect. Cell by cell, the misfolding spreads through the enteric nervous system.
Step 3 — The Highway
Then the clamps find the vagus nerve. And they climb. Via a process of retrograde transport, misfolded alpha-synuclein seeds travel upward along the vagal fibres — from the gut, through the brainstem, into the midbrain, and eventually to the cortex.
The first port of call is the dorsal motor nucleus of the brainstem. This correlates precisely with the earliest non-motor symptoms of Parkinson’s — sleep disturbances, depression, constipation, loss of smell — symptoms that often appear years before the tremor.
Eventually, the seeds reach the substantia nigra. Dopamine-producing neurons die. The motor symptoms begin.
By the time you see the tremor, you’re looking at the end of a very long story that started in the gut.
The Vagotomy Evidence: The Accidental Human Trial
Here is where the science becomes genuinely jaw-dropping.
In the mid-20th century, a common treatment for stomach ulcers was a procedure called a truncal vagotomy — surgically severing the vagus nerve to reduce stomach acid production. It was performed on hundreds of thousands of patients across multiple countries over several decades.
Epidemiological data later revealed something nobody was looking for.
Patients who had undergone a full truncal vagotomy showed a significantly reduced risk of developing Parkinson’s disease later in life.
Cut the highway between the gut and the brain. Parkinson’s risk drops.
This wasn’t a small study. This was large-scale population data. And what it tells us is that the vagus nerve isn’t just a communication channel between gut and brain. In a diseased gut environment, it becomes the anatomical bridge that allows pathology to travel from one to the other.
The medical establishment had accidentally run a massive human trial. And the result pointed directly at the gut as the origin of the disease.
This evidence is now considered among the strongest support for Braak’s Hypothesis. And it has profound implications for how we think about prevention.
Alzheimer’s: The Type 3 Diabetes Nobody Told You About
Parkinson’s isn’t the only neurodegenerative condition being reframed through the lens of metabolic and gut health.
Alzheimer’s disease — which affects over 900,000 people in the UK and is projected to rise to 1.6 million by 2040 — is increasingly understood through a framework called Type 3 Diabetes.
This isn’t fringe science. It’s the emerging consensus of nutritional neuroscience. And it changes everything about how we think about cognitive decline.
Here’s the mechanism.
Brain Insulin Resistance
Insulin isn’t just for managing blood sugar. In the brain, insulin is required to activate glucose transporters — specifically GLUT4 — in memory-critical regions like the hippocampus. When those regions become insulin resistant, they enter a state of localised energy crisis. ATP production drops. Mitochondria fail. Synaptic connections degrade.
The brain is starving. Not of calories. Of the ability to use the energy that’s already there.
The Sugar Rust — AGEs
Chronic hyperglycaemia produces a compound called methylglyoxal, the precursor to Advanced Glycation End-products (AGEs). These compounds cross-link with brain proteins, rendering them dysfunctional and triggering a destructive cycle of chronic neuroinflammation mediated by the brain’s immune cells — microglia.
Think of it as rust. Forming slowly. Inside your brain. Over years of elevated blood sugar.
The Overwhelmed Cleanup Crew
The Insulin-Degrading Enzyme (IDE) has two jobs. It clears excess insulin. And it clears amyloid-beta — the protein associated with Alzheimer’s plaques.
In a state of chronic hyperinsulinaemia, IDE is monopolised by excess insulin. It can’t do both jobs. Amyloid-beta accumulates freely.
The brain’s cleanup crew has been overwhelmed. Not by genetics. By metabolic dysfunction driven by decades of the wrong dietary inputs.
The Methionine-Acetylcholine Connection
There’s another mechanism connecting gut health to Alzheimer’s that rarely gets discussed. Your gut microbiome modulates the metabolism of methionine, an essential amino acid. Methionine is a precursor to SAM (S-adenosylmethionine), which is required for the synthesis of choline. And choline is the precursor for acetylcholine — the neurotransmitter most associated with memory and cognitive function.
Reduced acetylcholine is a primary hallmark of Alzheimer’s disease.
Gut dysbiosis disrupts this entire pathway. It doesn’t just affect your mood or your digestion. It starves your brain of the raw materials it needs for memory.
The Molecular Architecture of Brain Protection: The SCFA Fortress
So what stands between your gut and neurodegeneration?
Short-Chain Fatty Acids. SCFAs.
Specifically, the trinity of butyrate, propionate, and acetate — metabolites produced by your gut bacteria when they ferment dietary fibre. These aren’t just digestive byproducts. They are your brain’s primary architects of defence.
Here’s what they actually do.
Sealing the Gut Lining
SCFAs upregulate tight junction proteins — specifically occludin — in the gut epithelium. These proteins act as molecular bouncers, sealing the gaps between intestinal cells and preventing bacterial endotoxins from leaking into the bloodstream.
No leak. No LPS. No systemic endotoxaemia. No compromised blood-brain barrier.
Reinforcing the Blood-Brain Barrier
SCFAs don’t stop at the gut wall. They enter the systemic circulation and travel to the blood-brain barrier, where they bind to G protein-coupled receptors (GPR41/GPR43) on endothelial cells, signalling them to maintain structural integrity. They upregulate occludin here, too — specifically in the frontal cortex and hippocampus.
The fortress has two walls. SCFAs build and maintain both.
Activating the Master Antioxidant Defence
Propionate specifically activates the Nrf2 pathway — the body’s master antioxidant defence system. This armours the blood-brain barrier against oxidative erosion and reduces the expression of inflammatory receptors (CD14) that would otherwise trigger neuroinflammatory cascades.
Quenching Neuroinflammation
Once in the central nervous system, SCFAs block master inflammatory pathways — specifically NF-κB and MAPK. This calms microglial activation. In animal models, it has been shown to halt the degeneration of dopaminergic neurons and preserve motor function.
The SCFA fortress is not a nice-to-have. It is the primary molecular mechanism standing between your gut environment and your neurological future.
When SCFA production collapses — as it does on a modern Western diet low in fermentable fibre — both walls come down simultaneously.
The Tryptophan Hijack: When Your Gut Turns Against Your Brain
There’s another mechanism connecting gut inflammation to neurological damage that almost nobody is talking about.
Your gut microbiome controls the fate of tryptophan — the essential amino acid required for serotonin synthesis.
Under healthy conditions, dietary tryptophan is converted to serotonin (90-95% of which is produced in the gut) or 5-HTP, which crosses the blood-brain barrier for central nervous system serotonin production.
This is your mood, your sleep, your emotional resilience. All starting in your gut.
But when the gut is inflamed, a catastrophic diversion occurs.
Pro-inflammatory cytokines — TNF-α, IL-6, IFN-γ — activate an enzyme called IDO (indoleamine 2,3-dioxygenase). This enzyme hijacks tryptophan away from the serotonin pathway and diverts it into the kynurenine pathway instead.
The end products of this diversion are neurotoxic.
Quinolinic Acid (QUIN) — an excitotoxin that overstimulates NMDA receptors, triggering a calcium influx that destroys neuronal membranes
Your inflamed gut isn’t just failing to produce serotonin. It’s actively producing brain-damaging toxins from the same raw material that should have become your primary mood neurotransmitter.
This is the tryptophan hijack. And it runs silently in millions of people with chronic gut inflammation — most of whom have been told their depression, anxiety, or brain fog is a mental health issue, not a gut issue.
The Leaky Gut Pipeline: How Dysbiosis Becomes Neurodegeneration
Everything described above depends on one critical vulnerability: intestinal permeability—the leaky gut.
In a healthy gut, the epithelial lining is a masterwork of biological engineering. A single layer of cells secured by tight junction proteins — occludin and claudin — that act as molecular bouncers. Nutrients in. Pathogens out.
When the microbiome shifts into dysbiosis — an imbalance caused by processed foods, refined sugar, antibiotics, alcohol, and chronic stress — several things happen simultaneously.
Beneficial bacteria that produce mucins (the protective mucus layer) decline. The gut lining becomes more permeable. Gram-negative bacteria produce lipopolysaccharides (LPS) — bacterial endotoxins that can now breach the gut wall and enter the bloodstream.
This is systemic endotoxaemia. And it creates a vicious cycle.
LPS in the bloodstream triggers systemic inflammation. That inflammation weakens the blood-brain barrier. LPS enters the brain and activates microglia via the TLR4/MyD88/NF-κB pathway, thereby driving a self-sustaining cycle of neuroinflammation. The NLRP3 inflammasome — a multi-protein complex that initiates inflammatory cell death — is activated. Dopaminergic neurons die.
The leaky gut pipeline doesn’t just connect your gut to your brain. It is the mechanism by which a damaged microbiome becomes a damaged nervous system over time.
The gut is the source. The vagus nerve is the highway. The brain is the destination.
The Wrecking Crew vs The Fortress: What You’re Feeding Every Day
Your daily dietary choices are either to build the SCFA fortress or to send in the wrecking crew.
Here’s what each side looks like.
🔴 The Wrecking Crew
Refined Sugar and Processed Carbohydrates Drive hyperglycaemia and hyperinsulinaemia. Monopolise IDE. Allow amyloid-beta to accumulate—fuel pro-inflammatory bacterial species. Collapse SCFA production.
Gluten triggers the release of zonulin — a protein that physically disassembles the tight junction proteins of the gut lining. Leaky gut by design. This is the mechanism. It is not a wellness industry myth.
Ultra-Processed Food Strips the diet of fermentable fibre — the substrate your gut bacteria need to produce SCFAs. Without fibre, the architects have no materials. The fortress crumbles.
Alcohol directly damages the gut lining, disrupts the microbiome, drives LPS translocation, and compromises the blood-brain barrier. The gut-brain connection in alcohol recovery is a subject I’ve written about extensively — because it’s personal, and because the science is unambiguous.
Fermentable Fibre Vegetables, legumes, oats, resistant starch. This is the raw material for butyrate-producing bacteria — Faecalibacterium prausnitzii, Roseburia intestinalis. No fibre, no SCFAs. No SCFAs, no fortress.
Polyphenols: berries, dark chocolate, green tea, olive oil, herbs and spices. Polyphenols enhance SCFA production AND inhibit the IDO enzyme — shutting down the tryptophan hijack before it starts. They are simultaneously prebiotic fuel and neurological protection.
Omega-3 Fatty Acids: Oily fish, flaxseed, walnuts. Suppress intestinal inflammation, support SCFA-producing bacteria, and protect the serotonin pathway by keeping IDO dormant.
Fermented Foods: Sauerkraut, kimchi, kefir, live yoghurt. Increase microbiome diversity — your neurological insurance policy. Specific strains like Lactobacillus rhamnosus (JB-1 and HN001) and Bifidobacterium longum have been shown to directly activate the vagus nerve and alter GABA receptor expression in the brain.
Nutrient-Dense Proteins Provide choline (for acetylcholine and the methionine pathway) and tryptophan (for serotonin, when the IDO enzyme is kept dormant by the rest of the protocol).
Top-Down Toning: The Conscious Override
Diet — the bottom-up approach — is the foundation. But the gut-brain axis is bidirectional. And there are top-down practices that directly activate the parasympathetic nervous system and improve vagal tone, creating a feedback loop that protects both gut and brain simultaneously.
Cold Water Exposure Physically triggers the vagal dive reflex — an immediate systemic shift to parasympathetic dominance. Lower heart rate. Reduced cortisol. Calmer microglia. I use this daily. The science behind it is not optional reading for anyone serious about neurological longevity.
Breathwork Acts as a manual override for the autonomic nervous system. Controlled breathing through extended exhalation directly activates vagal efferent fibres — signalling safety to the enteric nervous system, improving insulin sensitivity, and reducing the inflammatory load that drives the tryptophan hijack.
Meditation operates at a systems level to calm microglial activation. Daily meditation practice reduces the neuroinflammatory baseline that, left unchecked, would progressively damage synaptic integrity.
HRV Tracking Heart Rate Variability — specifically the RMSSD metric (Root Mean Square of Successive Differences) — gives you a direct, objective measurement of vagal tone and parasympathetic activity. It is concrete proof that your interventions are working. Track it daily. Watch it improve. Your gut-brain highway is getting stronger in real time.
FAQ: The Questions I Know You’re Already Asking
Can diet actually prevent Parkinson’s disease?
There is no randomised controlled trial proving that specific dietary interventions prevent Parkinson’s in humans. What we have is a rapidly growing body of mechanistic evidence showing that gut health directly determines the biological conditions that precede neurodegeneration — often by 10 to 20 years. The mechanism is established. The intervention window is real. The vagotomy data are real. What you choose to do with that information is your call.
My GP has never mentioned any of this. Is it fringe?
It is being studied at Stanford, King’s College London, and the Mayo Clinic. It is published in Nature Neuroscience, Gut, and the Journal of Parkinson’s Disease. It is the subject of the MAMS EJS ACT-PD trials — the most sophisticated multi-arm clinical trials in neuroscience in 2025. It is not fringe. Your GP’s curriculum hasn’t caught up. That gap is what I’m here to close.
Is it too late if I’m already in my 40s or 50s?
The gut lining regenerates completely every few days. Microbiome composition shifts measurably within weeks of dietary change. The brain has extraordinary neuroplasticity. It is never too late to start. But the earlier you start, the longer the protective period you’re creating. The 20-year silent window cuts both ways — which means the next 20 years of what you eat matter more than most people will ever be told.
What about genetics?
Genetics loads the gun. Lifestyle pulls the trigger. For the vast majority of neurodegenerative disease risk, the gut environment determines whether a genetic predisposition becomes a clinical reality. The NLRP3 inflammasome, the TLR4 pathway, the IDO enzyme — these are not genetic inevitabilities. They are biological switches that your daily choices either activate or suppress
What’s the most important thing I can do right now?
Remove the wrecking crew first—Gluten, refined sugar, ultra-processed food. The gut lining cannot begin to heal while zonulin is continuously disassembling it. Week one of the 30-Day Reset is always about clearing the field before building the fortress.
The 30-Day Reset: Building Your Neurological Fortress
The protocol is simple. The discipline is the hard part.
📅 Week 1 — Remove the Wrecking Crew gluten and refined sugar. Ultra-processed food is out. Alcohol out. Watch what happens to your gut, your sleep, your mental clarity, and your brain fog within seven days. You’ll have your first data point.
📅 Week 2 — Flood with Fibre and Polyphenols. Every meal contains plants. Colour, variety, volume. Aim for 30 different plant species across the week — research shows this level of diversity dramatically shifts microbiome composition toward SCFA-producing species. Your gut bacteria are rebuilding the fortress.
📅 Week 3 — Reinoculate with Ferments Daily sauerkraut, kimchi, or kefir. This is where microbiome diversity begins to compound. Introduce the vagal-stimulating strains. Watch your RMSSD score start to climb.
📅 Week 4 — Repair and Audit: How’s the gut? The mood? The brain fog? The energy? The clarity? You have four weeks of biological data. You don’t need me or anyone else to tell you it’s working. Your body will be telling you loud and clear.
What’s Coming Next: The Bottom-Up Thesis
I’m going to be straight with you.
Everything in this article represents the tip of a very deep research process I’m currently embedded in.
The gut-brain-neurodegeneration connection — the bottom-up thesis that your gut is either building your brain or destroying it — is the subject of a book I’m developing. It goes deeper than anything currently on the market. Into the molecular origami of protein misfolding. Into the NLRP3 inflammasome and the toxic cascade. Into the 2025 clinical landscape of disease-modifying therapies. What Braak’s Hypothesis means not just for Parkinson’s but for the full spectrum of neurodegenerative conditions.
The research is ongoing. The book is coming.
If you want to be the first to know when it lands — and to get access to the research, protocols, and thinking as it develops — make sure you’re on the list.
The 30 Day Reset is not a diet. It is a complete biological overhaul for anyone who is wired, tired, and done with feeling like shite. The 30-Day Reset is a 160+ page military-grade systems reboot for the over-35s. Four pillars. Eat, sleep, move, mind. One month to strip out the industrial poison, reset your dopamine pathways, silence Bob, and rebuild the machine that’s been running on the wrong fuel for decades. Not a diet. Not a programme. A complete…
Your GP has had less than a week of training on gut and nutritional health. The system they were trained in has a blind spot the size of a motorway.
But you’ve just read the science. The vagotomy data. The Braak Hypothesis. The SCFA fortress. The tryptophan hijack. The Type 3 Diabetes framework. The 20-year silent window.
You now know more about the gut-brain connection and its role in neurodegeneration than most people will ever be told by anyone in a clinical setting.
The question is never what you know. It’s what you do with it.
Your gut is either building your brain or dismantling it. Every single day. Based on what you eat.
That’s not a scare tactic. That’s the machine. And now you know how it works.
👇 Drop a comment below. Has this changed how you think about gut health and brain disease? Has anyone in your family been affected by Parkinson’s or Alzheimer’s? I want to hear from you.
Ian Callaghan is a nutritional strategist, mindset coach, and author based in the UK. His work sits at the intersection of metabolic health, gut biology, and neurological longevity. He is the author of Fix Your Metabolism and The 30-Day Reset, and is currently deep in research for a groundbreaking new book on the bottom-up thesis of neurodegeneration.
Used to monitor number of Google Analytics server requests when using Google Tag Manager
1 minute
_gid
ID used to identify users for 24 hours after last activity
24 hours
_ga_
ID used to identify users
2 years
_gali
Used by Google Analytics to determine which links on a page are being clicked
30 seconds
_ga
ID used to identify users
2 years
__utmx
Used to determine whether a user is included in an A / B or Multivariate test.
18 months
__utmv
Contains custom information set by the web developer via the _setCustomVar method in Google Analytics. This cookie is updated every time new data is sent to the Google Analytics server.
2 years after last activity
__utmz
Contains information about the traffic source or campaign that directed user to the website. The cookie is set when the GA.js javascript is loaded and updated when data is sent to the Google Anaytics server
6 months after last activity
__utmc
Used only with old Urchin versions of Google Analytics and not with GA.js. Was used to distinguish between new sessions and visits at the end of a session.
End of session (browser)
__utmb
Used to distinguish new sessions and visits. This cookie is set when the GA.js javascript library is loaded and there is no existing __utmb cookie. The cookie is updated every time data is sent to the Google Analytics server.
30 minutes after last activity
__utmt
Used to monitor number of Google Analytics server requests
10 minutes
__utma
ID used to identify users and sessions
2 years after last activity
_gac_
Contains information related to marketing campaigns of the user. These are shared with Google AdWords / Google Ads when the Google Ads and Google Analytics accounts are linked together.